A 10-year-old MN mixed breed dog presented for renal failure from a referral hospital. In-house blood chemistry revealed hypoalbuminemia, high ALP, azotemia, hypercalcemia, and hyperphosphatemia.
A 10-year-old MN mixed breed dog presented for renal failure from a referral hospital. In-house blood chemistry revealed hypoalbuminemia, high ALP, azotemia, hypercalcemia, and hyperphosphatemia.
Chronic degenerative renal insufficiency, glomerulonephritis, infectious (Leptospira sp., Dirofilaria immitis, Borrelia burgdorferi), immune-mediated, pyelonephritis, neoplasia (lymphoma, renal adenocarcinoma with metastases to the surrounding organs, adrenal mass such as adenocarcinoma, adenoma, or pheochromocytoma), nephrolithiasis, ureterolithiasis, or urolithiasis causing an obstruction and secondary renal failure.
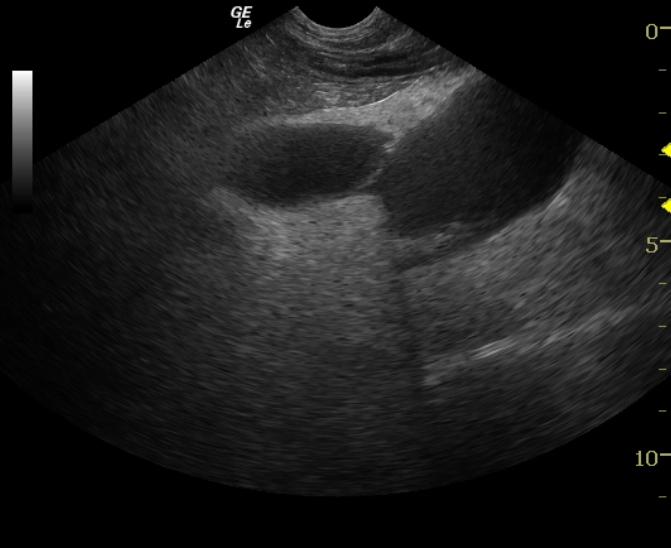
Mineralizing right adrenal mass invading the caudal vena cava.
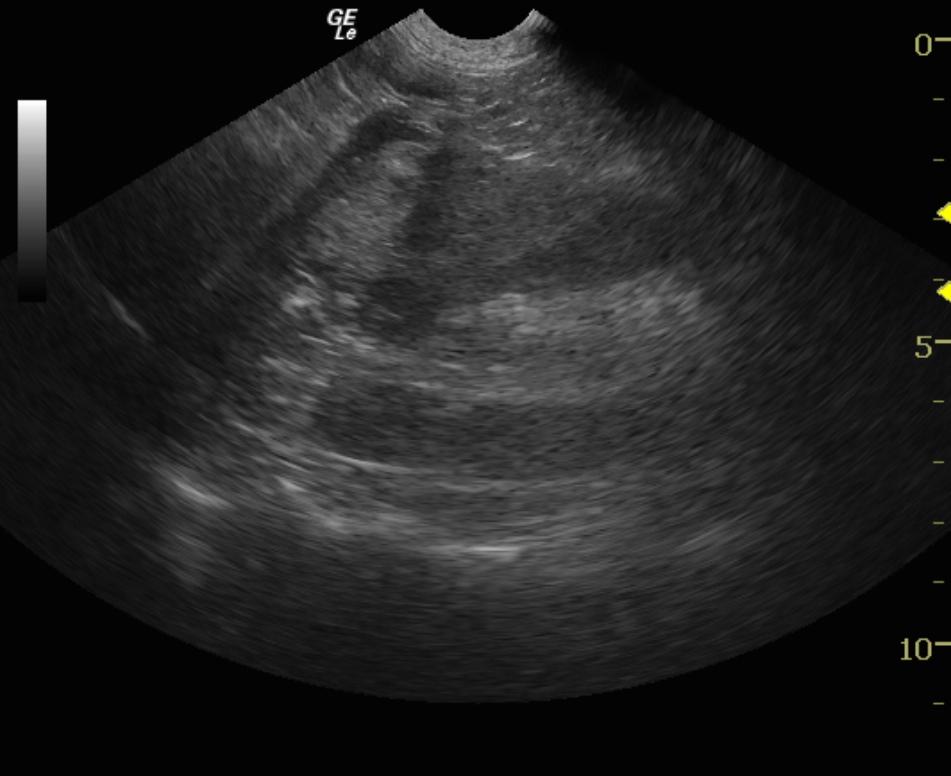
Both kidneys contained corticomedullary calculi. The right kidney presented significant chronic hydroureter with a ureter calculus at the mid to distal right ureter, an inflammatory adhesion pattern, and moderate pelvic dilation of 1.7cm. Free fluid was noted in the abdomen as well which was sampled and found to be serohemorrhagic. Azostix revealed significant azotemia of the free fluid, suspicious for ureter rupture. The right kidney presented moderate hydronephrosis. The left adrenal gland was normal size and contour. The right adrenal gland presented a mass which invaded the caudal vena cava. Mineralization was also present. The vena cava was nearly 80% obstructed, and is not considered resectable.