A 15-year-old FS DSH with was presented for decreased appetite and lethargy with a history of hypoalbuminemia, hypomagnesemia, and hypocalcemia. On physical examination weight loss, pyrexia, dehydration, icterus, and a grade III/VI heart murmur were present. Abnormalities on CBC and serum biochemistry were leukocytosis with a mature neutrophilia, monocytosis, non-regenerative anemia, azotemia, hyperphosphatemia, and hypocalcemia.
A 15-year-old FS DSH with was presented for decreased appetite and lethargy with a history of hypoalbuminemia, hypomagnesemia, and hypocalcemia. On physical examination weight loss, pyrexia, dehydration, icterus, and a grade III/VI heart murmur were present. Abnormalities on CBC and serum biochemistry were leukocytosis with a mature neutrophilia, monocytosis, non-regenerative anemia, azotemia, hyperphosphatemia, and hypocalcemia.
Icterus – prehepatic (IMHA, mycoplasmosis, toxins), post-hepatic (cholecystitis/rupture/bile duct obstruction secondary to neoplasia, pancreatitis, duodenal IBD/neoplasia/foreign body). Azotemia – chronic kidney disease, pyelonephritis. Heart murmur – cardiomyopathy, valve insufficiency, physiological (anemia).
Malignant B cell neoplasm deriving from an abdominal lymph node with multifocal amyloid deposition.
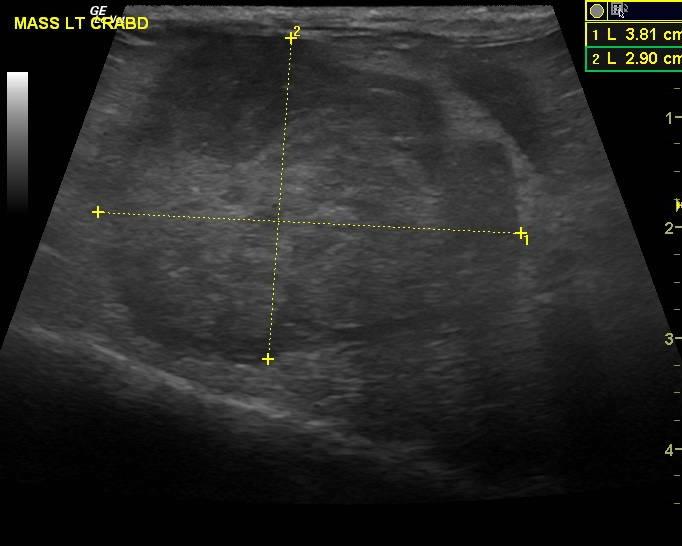
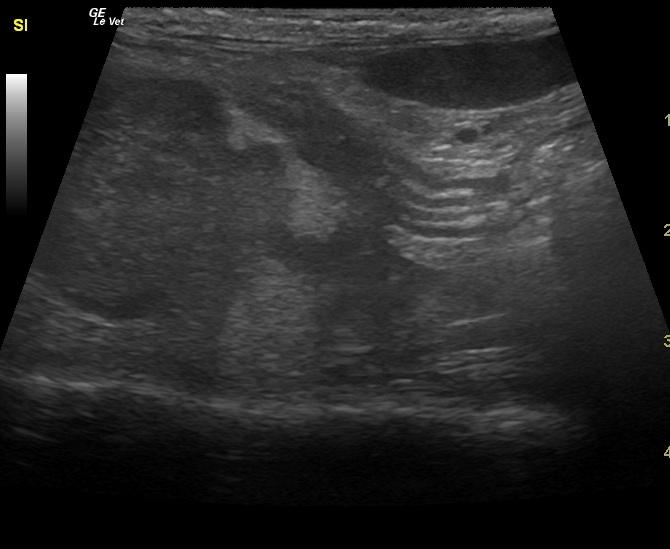
The patient had been treated with I.V. fluids, Pepcid, pain medication, KCl, Baytril, and amoxicillin. After responding to treatment, the patient was discharged only to re-present for vomiting, lethargy,progressive weight loss, and acute change in mentation. Physical examination found that the original abdominal mass was enlarged, now felt irregular, and encompassed the majority the patient’s abdomen. A new mass was also discovered in the caudal abdomen on palpation. Abnormalities on recheck blood work were leukocytosis, neutrophilia with 1+ toxic changes and resolved monocytosis, Hct 15% (normocytic, normochromic non-regenerative anemia,) TP 7.2 g/dl, azotemia, BUN 126 mg/dl, creatinine 6.7 g/dl, Phos 14.3 mg/dl, and Ca 7.3. Follow-up ultrasound revealed persistence of the ileocecocolic mass, which is likely of lymph node origin. It now measured 4.8 x 1.97 cm. A minor amount of free fluid was noted at this point likely owing to lymphatic strangulation at the mesenteric root. Note: The clinical renal profile was caused by ureterolithiasis of the left ureter and secondary left hydronephrosis. The heart murmur was a simple physiological flow turbulence. The pathologist also felt that amyloid was likely in the kidneys, creating the urolithiasis and subsequent acute change in mentation from severe azotemia.