A 10-year-old neutered male Pomeranian dog was presented for evaluation of severe vomiting, inappetence, diarrhea, and lethargy. A cystotomy had been done two years ago. The patient only eats table food, and is on no specific medications. The only significant finding on physical examination was mild cranial abdominal discomfort. Inappropriate SG (1.023), 1+ protein, ands 1+ bilirubin was present on urinalysis. Neutrophilia with a left shift was present on CBC.
A 10-year-old neutered male Pomeranian dog was presented for evaluation of severe vomiting, inappetence, diarrhea, and lethargy. A cystotomy had been done two years ago. The patient only eats table food, and is on no specific medications. The only significant finding on physical examination was mild cranial abdominal discomfort. Inappropriate SG (1.023), 1+ protein, ands 1+ bilirubin was present on urinalysis. Neutrophilia with a left shift was present on CBC. On serum biochemistry, all of the following values were elevated: proteins, ALT, ALP, amylase, phosphate, glucose, BUN, creatinine, and cPL.
GI signs – pancreatic disease (acute pancreatitis, neoplasia), GI disease (foreign body with obstruction/perforation, neoplasia), peritonitis. Azotemia – chronic kidney disease, acute renal failure, obstructive uropathy. Elevated liver values – acute hepatitis, trauma, abscess, neoplasia.
The renal parameters on blood chemistry were more dramatic then the ultrasonographic appearance of the kidneys themselves. Therefore, a prerenal component such as pancreatitis is likely complicating the presentation. However, it is also possible that if the patient has moved renal calculi from the kidneys to the bladder, causing the aggressive vomiting episode and discomfort.
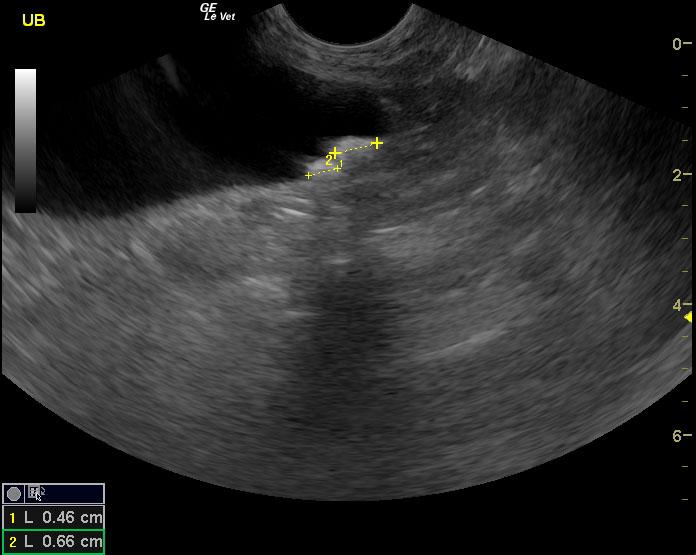
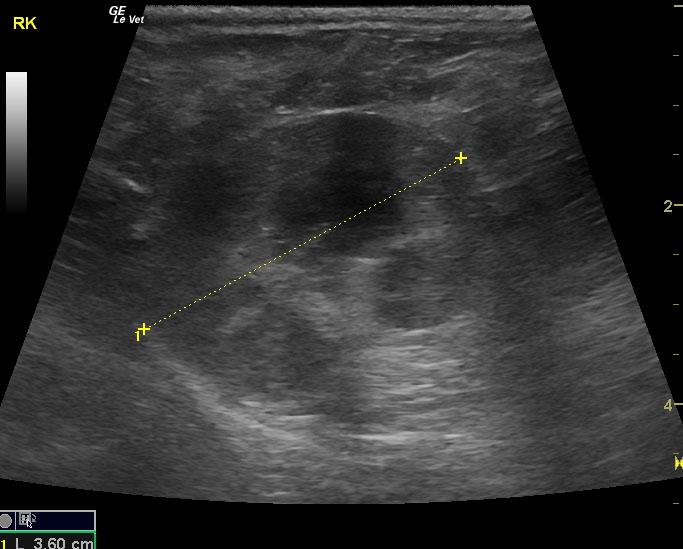
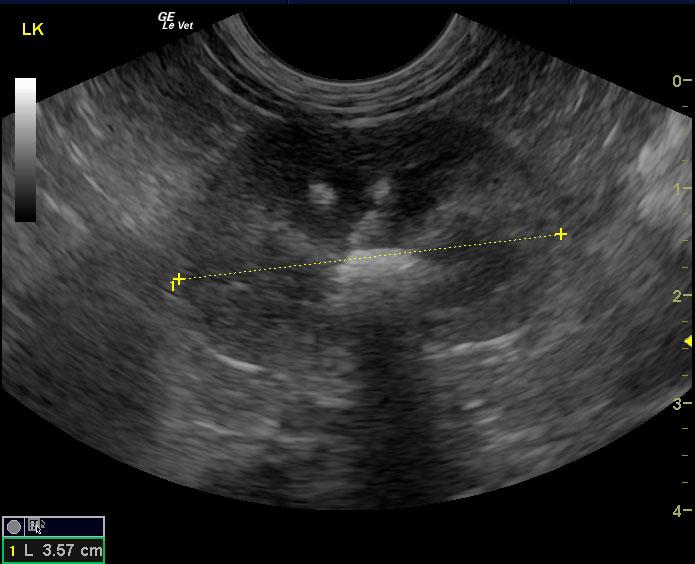
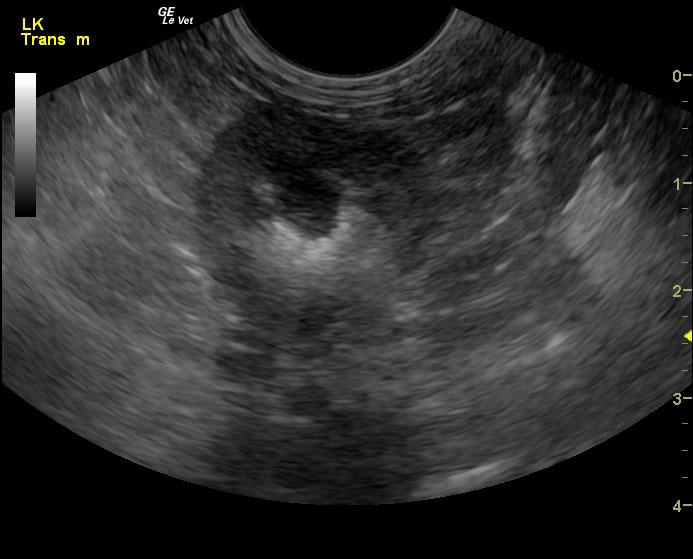
The urinary bladder, trigone and pelvic urethra presented normal wall thicknesses with anechoic urine and normal tone. Two shadowing calculi were noted in the trigonal region measuring 0.46 and 0.66 cm. No evidence of inflammatory or neoplastic changes were noted. The ureters were not visible and considered normal. The right kidney presented mild to moderate degenerative changes. The left kidney demonstrated mild degenerative changes, medullary calculi, and corticomedullary calculi. These stones were non obstructive at this time, but they are in position to displace into the ureters and urinary bladder. Slight pyelectasia was noted in the right kidney; occult urinary tract infection is likely an issue.