A 10-year-old SF DSH was presented for evaluation of oral ulcers and anorexia for several days. On physical examination, resistance to abdominal palpation was present. Urinalysis showed isosthenuria, 1+ protein, and trace hematuria. Abnormalities on serum biochemistry were azotemia, hyperphosphatemia, and mild hyperkalemia.
A 10-year-old SF DSH was presented for evaluation of oral ulcers and anorexia for several days. On physical examination, resistance to abdominal palpation was present. Urinalysis showed isosthenuria, 1+ protein, and trace hematuria. Abnormalities on serum biochemistry were azotemia, hyperphosphatemia, and mild hyperkalemia.
Renal – acute kidney disease, chronic kidney disease, pyelonephritis, renoliths, ureteroliths, lymphoma, infarction.
U/S guided FNA (25 gauge needle) of the kidneys and liver would be indicated in this case to differentiate between pyelonephritis and renal lymphoma. Aggressive empirical treatment for pyelonephritis would be warranted. If minimal sediment is present in the urine, then this presentation is likely most consistent with renal lymphoma.
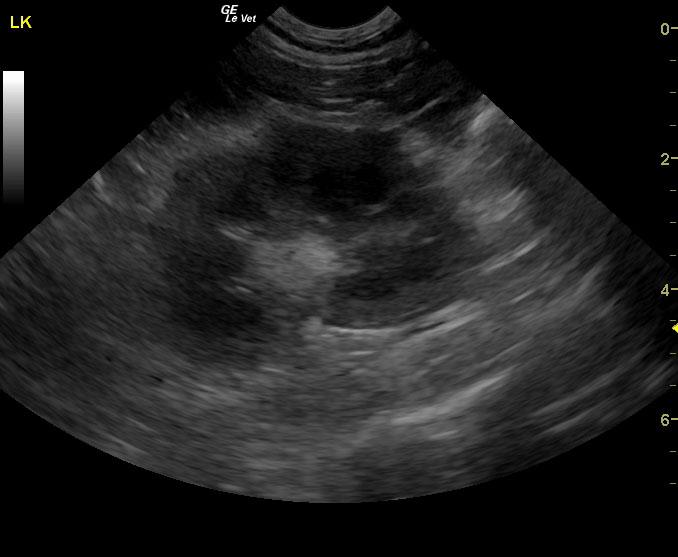
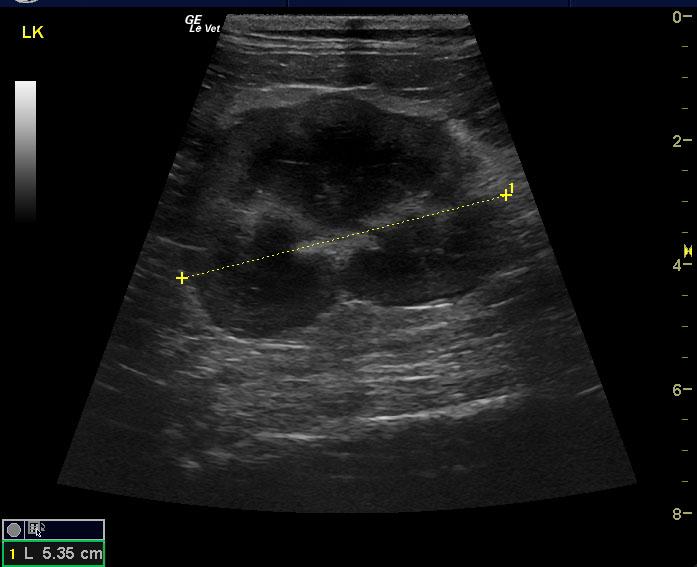
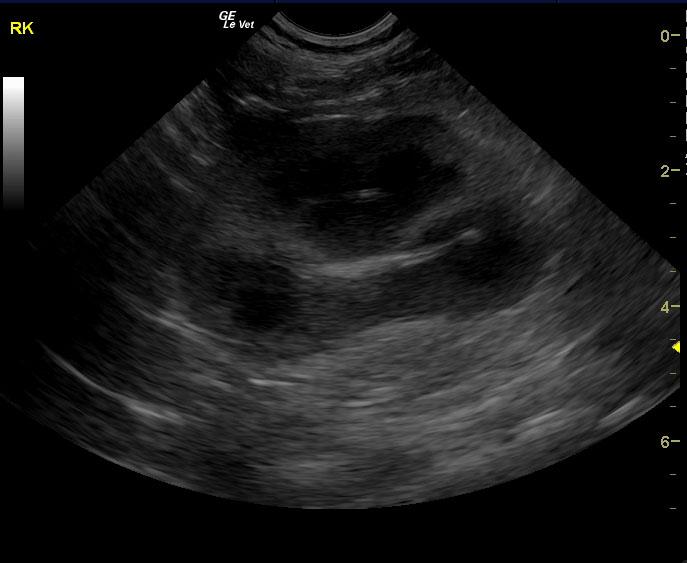
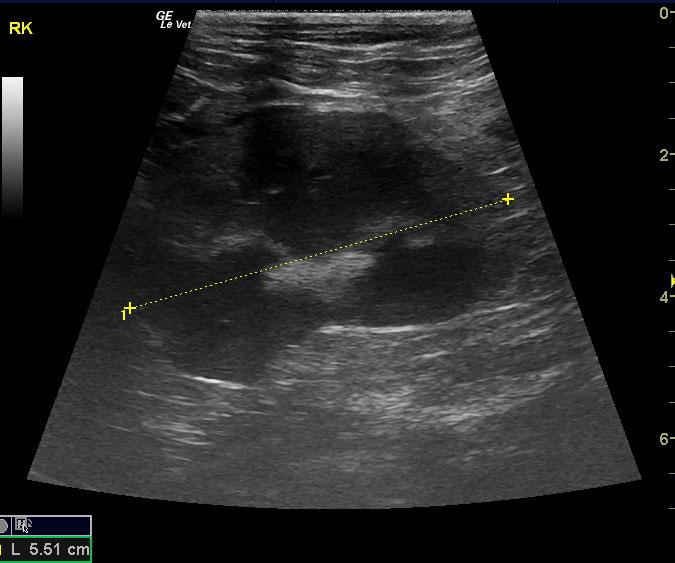
The left kidney was enlarged with significantly irregular contour. There was a pericapsular inflammatory pattern, slight, hypoechoic subcapsular rim, and pyelectasia (0.44 x 0.77 cm). The right kidney demonstrated similar, milder changes, and was enlarged.