The patient is a feline DSH, SF, 17 years old. Clinical exam findings: Acute onset weakness and fever on PE (105 F), client reports hyperexia and acute onset stranguria, pollakiuria. Recently increased Methimazole due to ongoing elevation in T4. Recent COHAT with extraction, mild suture reaction, no intra-oral inflammation currently. History of suspected pyelonephritis treated with 6 week course Clavamox with 2 negative cultures. Altered CBC/Chem/UA values: Today- CBC- WBC= 24 (5.5-19), Lym= 1.26 (1.5-14), Neut= 21.4 (2.5-14). Chemistry: BUN= 57 , Creatinine= 3.4 (0.3-2.1). Systemic BP WNL.
The patient is a feline DSH, SF, 17 years old. Clinical exam findings: Acute onset weakness and fever on PE (105 F), client reports hyperexia and acute onset stranguria, pollakiuria. Recently increased Methimazole due to ongoing elevation in T4. Recent COHAT with extraction, mild suture reaction, no intra-oral inflammation currently. History of suspected pyelonephritis treated with 6 week course Clavamox with 2 negative cultures. Altered CBC/Chem/UA values: Today- CBC- WBC= 24 (5.5-19), Lym= 1.26 (1.5-14), Neut= 21.4 (2.5-14). Chemistry: BUN= 57 , Creatinine= 3.4 (0.3-2.1). Systemic BP WNL. U/A- U.S.G.= 1.020, NSF, sent out for culture. B/W performed a week ago- CBC WNL (WBC= 9, Neut= 5.8), Chemistry- BUN= 42, Creatinine = 2.2.
06-00107 Gracie R Cystic calculus *BK*—NEEDS CDX————
History
DX
Sampling
None
Sonographic Differential Diagnosis
The bladder stone appears stable at this time. However, if pyelonephritis is an issue, 72 hour IV fluid protocol would be ideal or direct cystotomy with stone removal as the calculus would be difficult to pass. Another option would be ultrasound-guided pyelocentesis of the right kidney, drainage and culture.
Image Interpretation
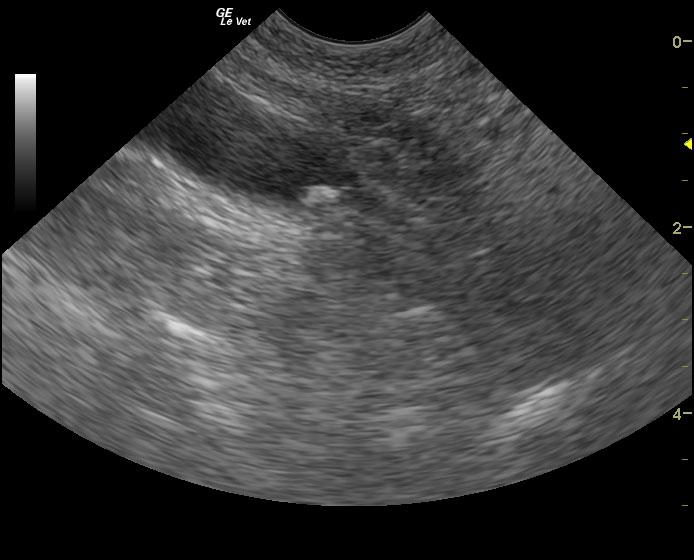
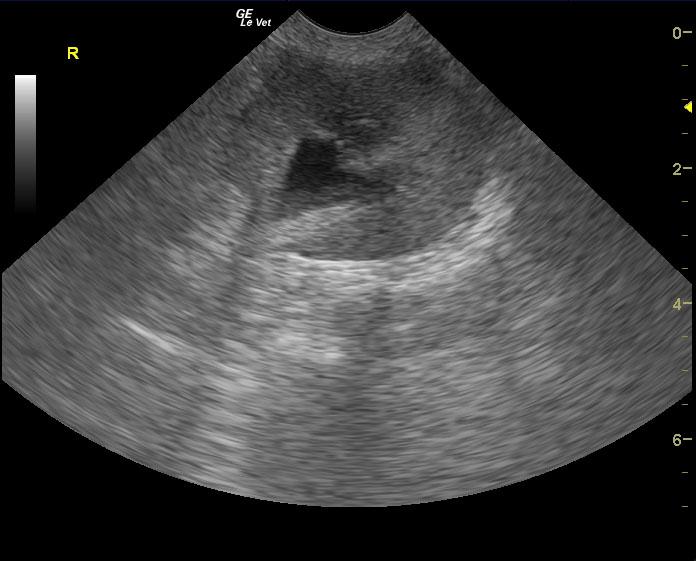
The bladder in this patient presented normal structure. However, a 0.5 cm calculus was located at the cystourethral junction, yet not embedded within it at the time of sonogram. Dependent debris was also noted in the urinary bladder. The patient has likely passed the calculus from the right kidney with secondary blood clots and/or pyelonephritis in the right renal pelvis. The kidneys presented moderate degenerative changes with thickened cortices and an interstitial nephrosis pattern. Dystrophic mineralization was noted in both kidneys. Slight pyelectasia was noted in the left kidney. The patient may have passed the calculus recently. The right kidney presented moderate pelvic dilation at 1.0 cm with dystrophic mineralization. Dependent debris was noted in the renal pelvis. This is suggestive of pyelonephritis. Ultrasound-guided drainage and culture of the right renal pelvis would be ideal in this case.
Outcome
Hospitalized on IVF and oral antibiotics since the initial sonogram and was febrile for 4 days, but now improved. Eating well. Recent bloodwork shows no improvement in renal values. Urine culture had no growth. Altered CBC/Chem/UA values: 5/22- Chemistry: BUN= 58, Creatinine 3.5.
Video
Patient Information
Blood Chemistry
- BUN high
- Creatinine, High
CBC
- Lymphocytes, Low
- Neutrophils, High
- WBC, High
Clinical Signs
- Fever
- Pollakiuria
- Polyphagia
- Stranguria
- Weakness
Images