A 16-year-old MI Lhasa was presented for evaluation. Laboratory work showed glycosuria, proteinuria, severe leukocytosis, azotemia, and hypercalcemia. Hypertension (240) was also present.
A 16-year-old MI Lhasa was presented for evaluation. Laboratory work showed glycosuria, proteinuria, severe leukocytosis, azotemia, and hypercalcemia. Hypertension (240) was also present.
Hypercalcemia of malignancy
Renal – acute kidney injury, pyelonephritis, abscess, neoplasia
Intestinal abscess/granuloma with focal peritonitis
Peritonitis
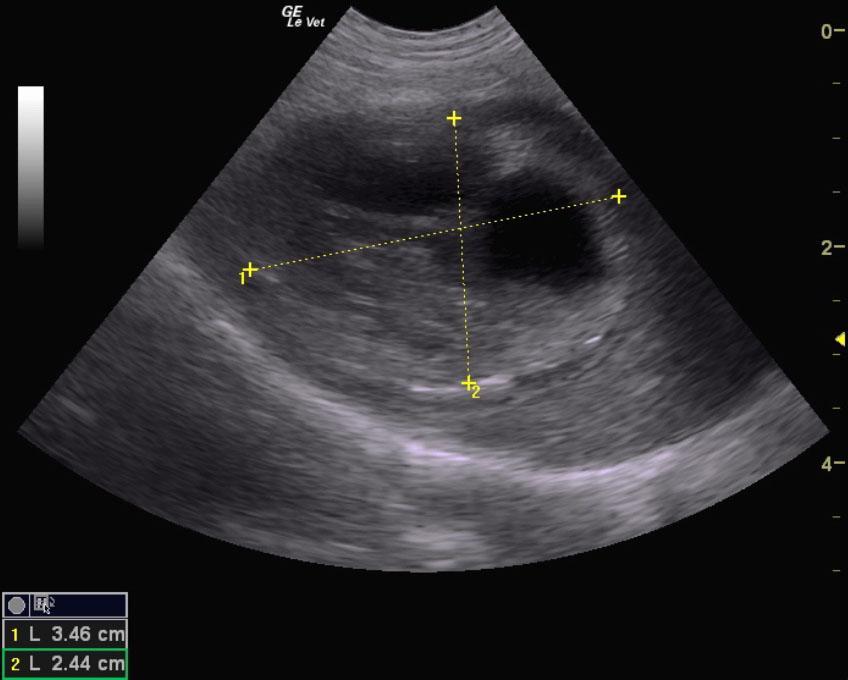
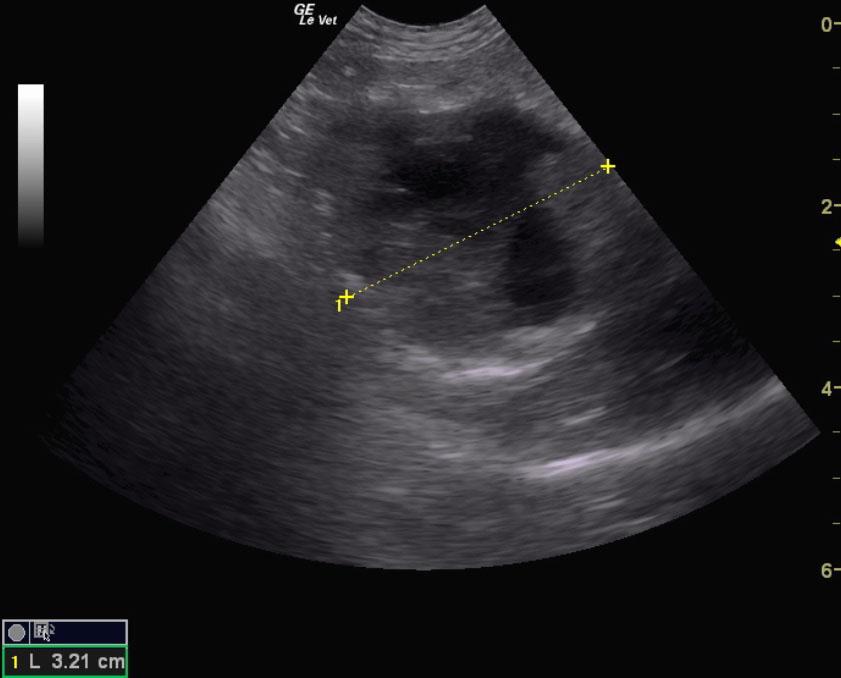
Mural duodenal mass, possible abscessing carcinoma or mural abscess.
Minor, regional pancreatic inflammation.
Billroth gastrointestinal reconstruction is likely necessary. Neutering, cystotomy, culture and sensitivity and gastrointestinal reconstruction is recommended in this patient. It may be possible to drain the mural lesion in the upper duodenum without resecting. However, it depends if this is underlying abscess with inflammatory disease, abscessing carcinoma or lymphoma. Guarded prognosis.
ADD??? Testicular abscess or neoplasia with BPH prostate. Multiple bladder calculi.
Some retention of ingesta was noted in the stomach. A mural duodenal mass was noted and measured 3.5x 2.5×3.2 cm with echogenic debris. This appears to be deriving from the muscularis and appears to be unilateral. This is consistent with a duodenal abscess or possible abscessing neoplasia such as carcinoma. Surgical intervention is recommended along with likely Billroth gastrointestinal reconstruction.
The pancreas presented a minor amount of remodeling with echogenic inflammatory pattern adjacent to a mural duodenal mass.