A 10-year-old intact M Vizsla dog was presented for evaluation of one week duration of progressive hacking, non-productive cough. On physical examination increased respiratory sounds, irritable trachea, and mild dental disease was present. CBC was within reference range. On thoracic radiographs marked cardiomegaly with a globoid cardiac silhouette, marked tracheal elevation, and a mild interstitial lung pattern was evident.
A 10-year-old intact M Vizsla dog was presented for evaluation of one week duration of progressive hacking, non-productive cough. On physical examination increased respiratory sounds, irritable trachea, and mild dental disease was present. CBC was within reference range. On thoracic radiographs marked cardiomegaly with a globoid cardiac silhouette, marked tracheal elevation, and a mild interstitial lung pattern was evident.
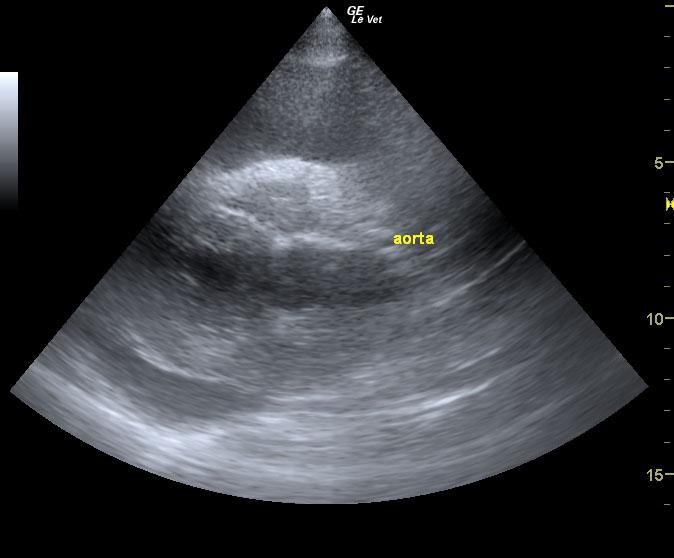
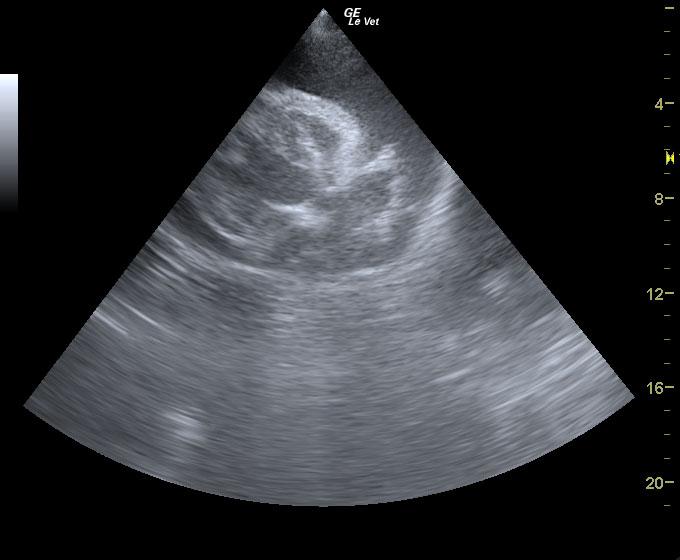
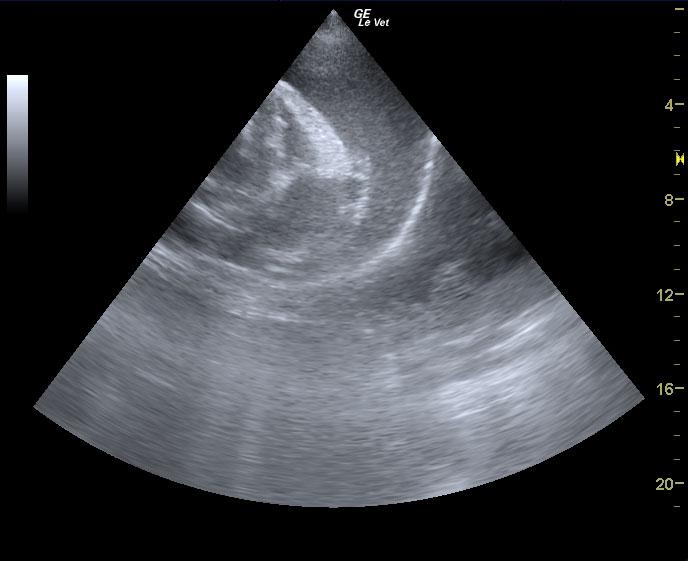
Suspected idiopathic pericardial effusion.
Right auricular mass cannot be definitively ruled out at this time. Recommend treatment for idiopathic pericardial effusion with a recheck in 2-4 weeks for a repeat scan. No medications are advised at this time unless pericardial is forming. Recommend cytology and culture of pericardial fluid.
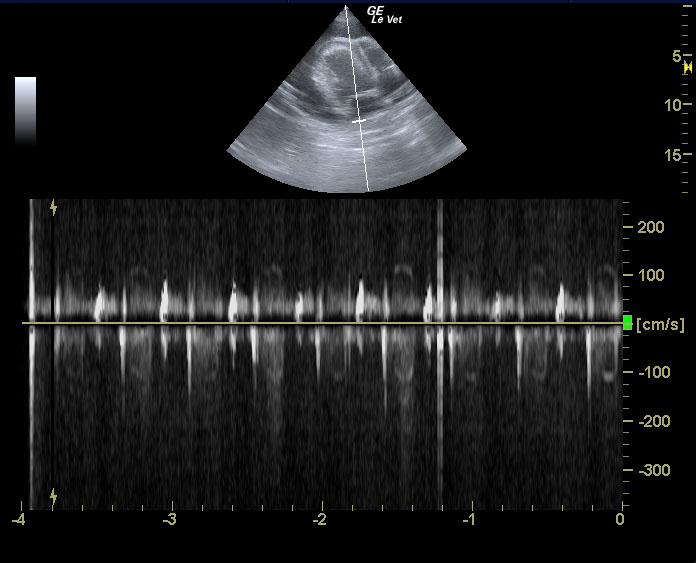
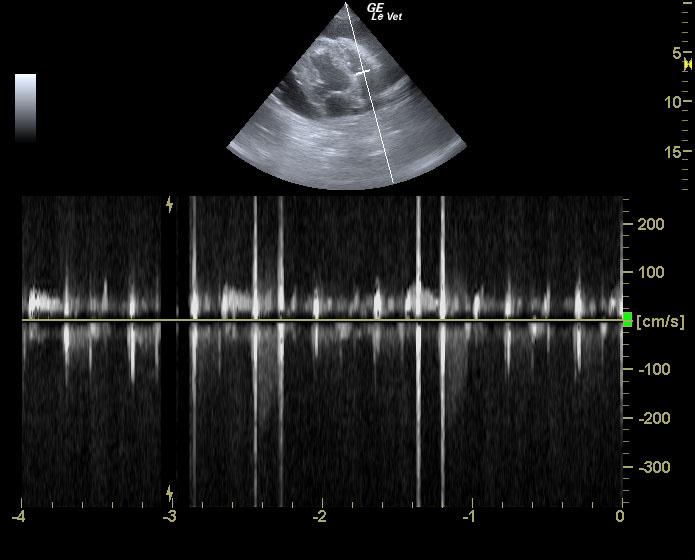
The LV was normal in diastole and systole. The fractional shortening (FS) was within normal limits indicating adequate systolic function. The EPSS (end point to septal separation) was also within normal limits (another indicator of adequate systolic function). The endocardial surface of all chambers was normal in echogenicity and smooth. The MV showed normal excursion and anatomy. There was no significant mitral insufficiency noted on Doppler. The LA was normal in size. The La/Ao ratio was within normal limits for the patient’s body weight. The RA appeared normal. The RV demonstrated normal thickness when compared to the LV (approx 1/3 of LV). No abnormalities of the TV were noted. There was no evidence of significant regurgitation or stenosis. The left and right ventricular outflow tracts were normal in appearance. The aortic outflow tract had normal flow dynamics with no evidence of aortic restrictions or post-valvular dilations. The aortic valve had normal anatomy and excursion. The MPA was normal in relation to the aorta (1:1) PA/Ao ratio). There were no heartworms noted in the visible portion of the pulmonic outflow tract. It had normal laminar patterns showing no evidence of stenosis or regurgitation. The PV was visualized and was normal. The myocardium throughout the heart was uniformly echogenic without evidence of significant fibrosis or infiltrative disease. There was marked pericardial effusion. 340 mls were drawn off. No right sided tamponade was visible. No right atrial masses or aortic base tumors were noted.