– 9 yr MN Doberman with history of hematuria for a few weeks now
– was neutered 1 year ago due to “prostate issues” but resovled once neutered
– rDVM performed urine culture on free flow sample which came up negative
– urine sediment struvites, RBC’s TNTC, no abnormal cells
– after antibiotic tx struvites resolved but hematuria persisted
– x-rays unremarkable
– 9 yr MN Doberman with history of hematuria for a few weeks now
– was neutered 1 year ago due to “prostate issues” but resovled once neutered
– rDVM performed urine culture on free flow sample which came up negative
– urine sediment struvites, RBC’s TNTC, no abnormal cells
– after antibiotic tx struvites resolved but hematuria persisted
– x-rays unremarkable
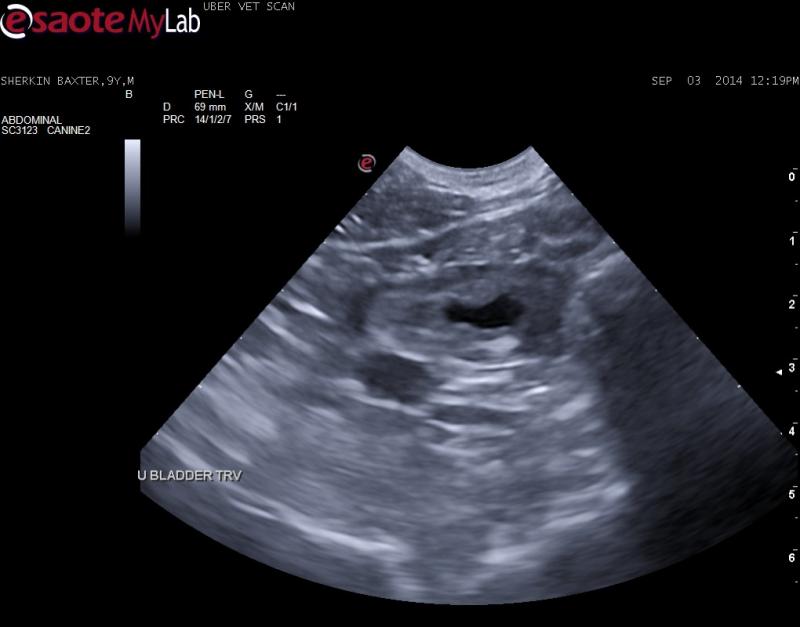
Ultrasound: apical wall thickening which I think is abnormal despite small UB due to lack of urine. Almost has polypoid cystitis-look but not quite. A hyperechoic body apears to be embedded in the wall – non-shadowing. No intraluminal uroliths or sand seen. Trigone, kidneys, prostate and medial iliac LN’s all appear normal. I have recommended a suction biopsy. Could this be an atypical TCC? Surgical options?

4 responses to “Apical Bladder Lesion”
This is likely a chronic
This is likely a chronic polypoid cystitis and that echogenic lesion is mural scarring if I had to do histopathological ultrasound but TCC possible so traumatic cath on this is the way to go.
http://sonopath.com/resources/interventional-procedures
TCC can look like this early but the echogenic change is not typical like TCC mineralization. This dog has likely been harboring infection for some time and will be tough to clear may have to pulse ABs. The bleed can come from fragile vessels in the wall (just remember you last angry bladder cystotomy) or deriving from the kidneys or even prostate/urethra depending on what they look like sonographically. You can power doppler the wall to assess vascularity. Traum cath for both histopath and culture go 6 weeks abs and recheck culture at 4-5 weeks and sonogram is what i would do to see any improvement or progression. Not surgical as its concentric and not resectable completely.
Check these chronic cystitis cases out on the basic search:
http://sonopath.com/members/case-studies/search?text=chronic+cystitis&species=All
Nice post:)
This is likely a chronic
This is likely a chronic polypoid cystitis and that echogenic lesion is mural scarring if I had to do histopathological ultrasound but TCC possible so traumatic cath on this is the way to go.
http://sonopath.com/resources/interventional-procedures
TCC can look like this early but the echogenic change is not typical like TCC mineralization. This dog has likely been harboring infection for some time and will be tough to clear may have to pulse ABs. The bleed can come from fragile vessels in the wall (just remember you last angry bladder cystotomy) or deriving from the kidneys or even prostate/urethra depending on what they look like sonographically. You can power doppler the wall to assess vascularity. Traum cath for both histopath and culture go 6 weeks abs and recheck culture at 4-5 weeks and sonogram is what i would do to see any improvement or progression. Not surgical as its concentric and not resectable completely.
Check these chronic cystitis cases out on the basic search:
http://sonopath.com/members/case-studies/search?text=chronic+cystitis&species=All
Nice post:)
The other possiblity for the
The other possiblity for the hyperechoic region would be a previous cystotomy.
The other possiblity for the
The other possiblity for the hyperechoic region would be a previous cystotomy.