A 14-year-old NM Abyssinian with a history of stage II chronic kidney disease, UTI, and idiopathic cystitis was presented for evaluation of stranguria, pollakuria, and inappropriate urination. Systolic blood pressure was elevated. Urinalysis showed SG 1.025 and pyuria. CBC, T4, and ProBNP were all normal. Abnormalities on serum biochemistry were azotemia, hyperglobulinemia, hypokalemia, and mild hyperglycemia.
Renal – chronic kidney disease, hypertensive nephropathy, potassium-losing nephropathy, renoliths, pyelonephritis, granulomatous nephritis
Bladder – bacterial cystitis, neoplasia, interstitial cystitis, uroliths, polyploid cystitis
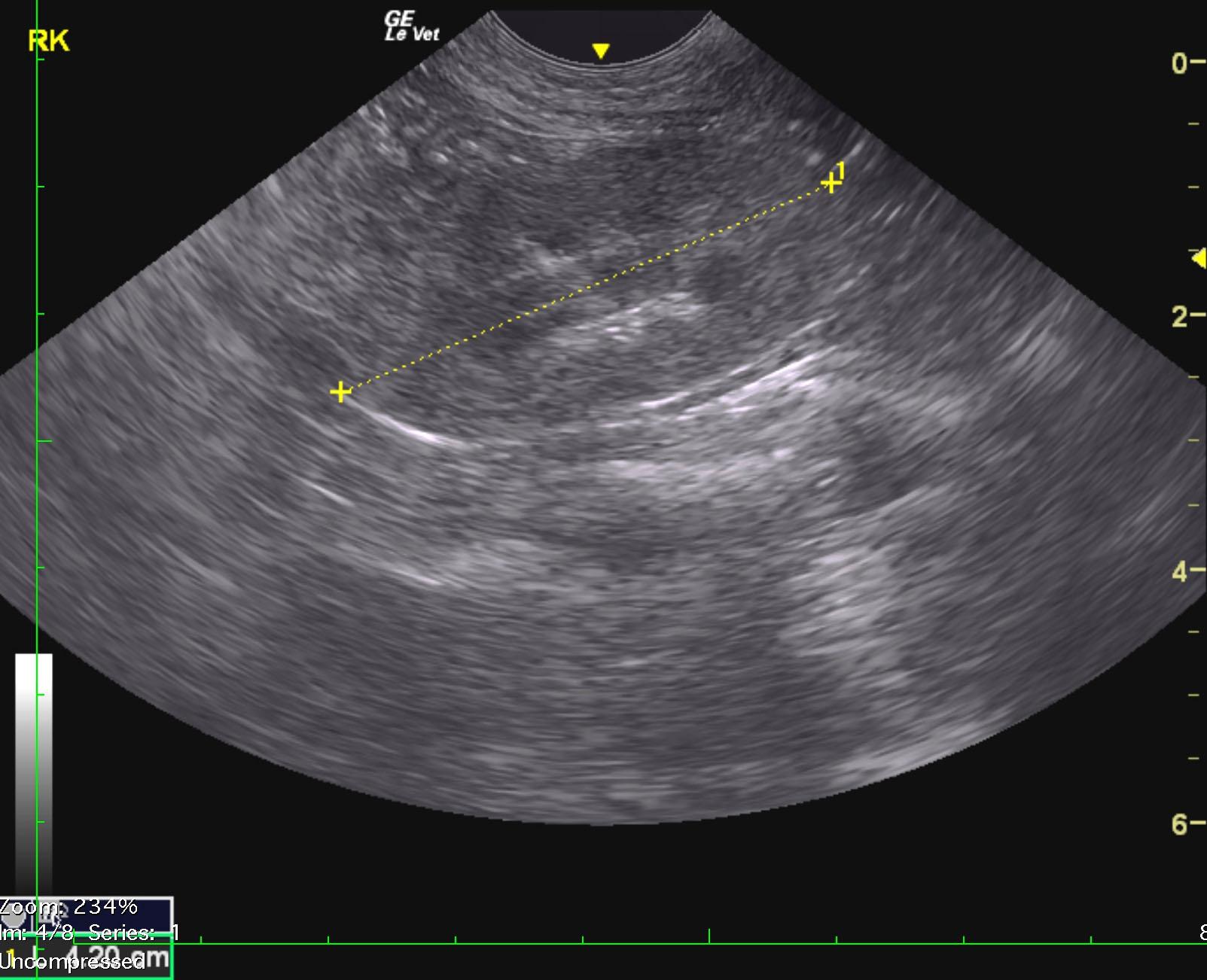
Chronic interstitial nephrosis renal pattern.
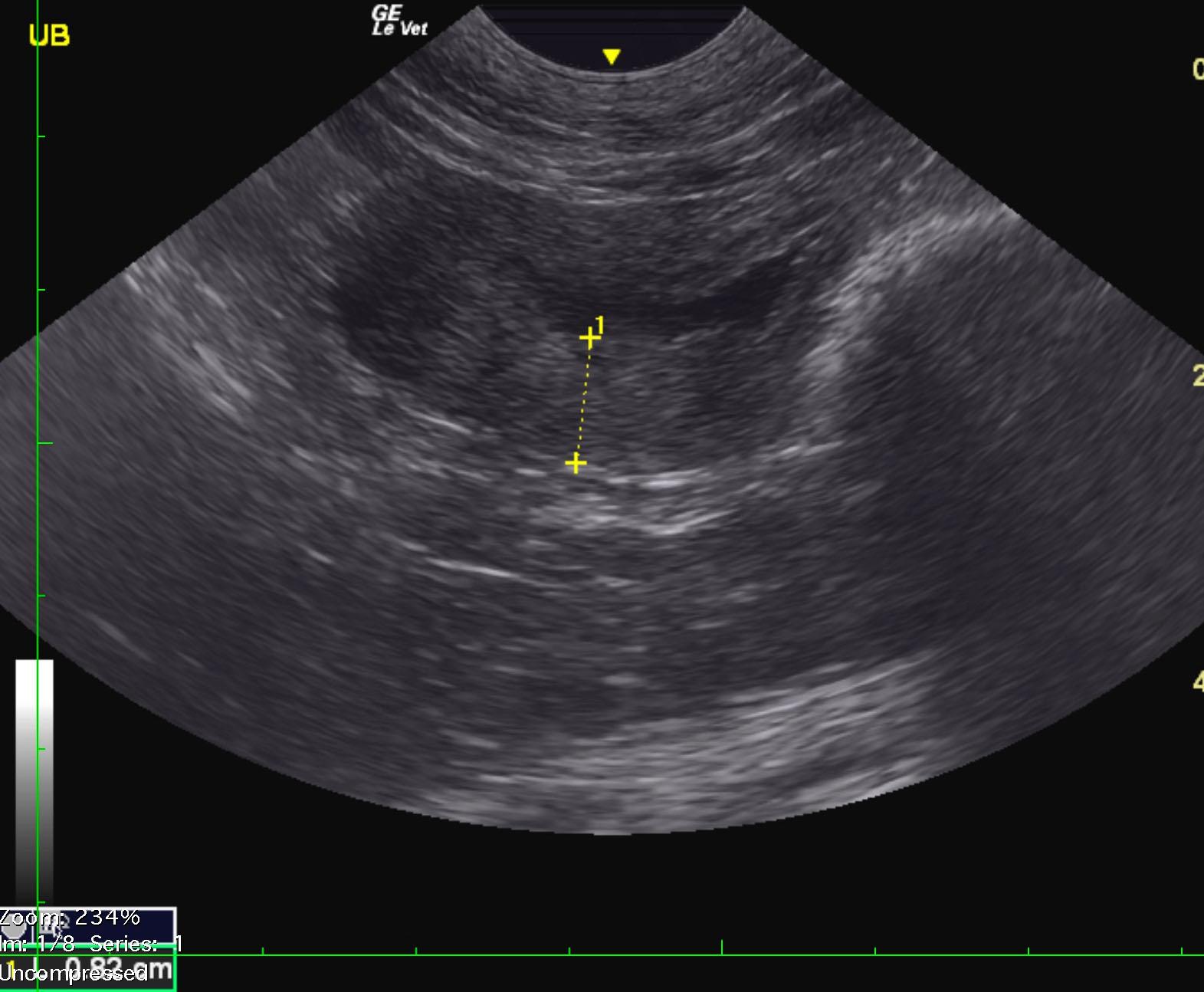
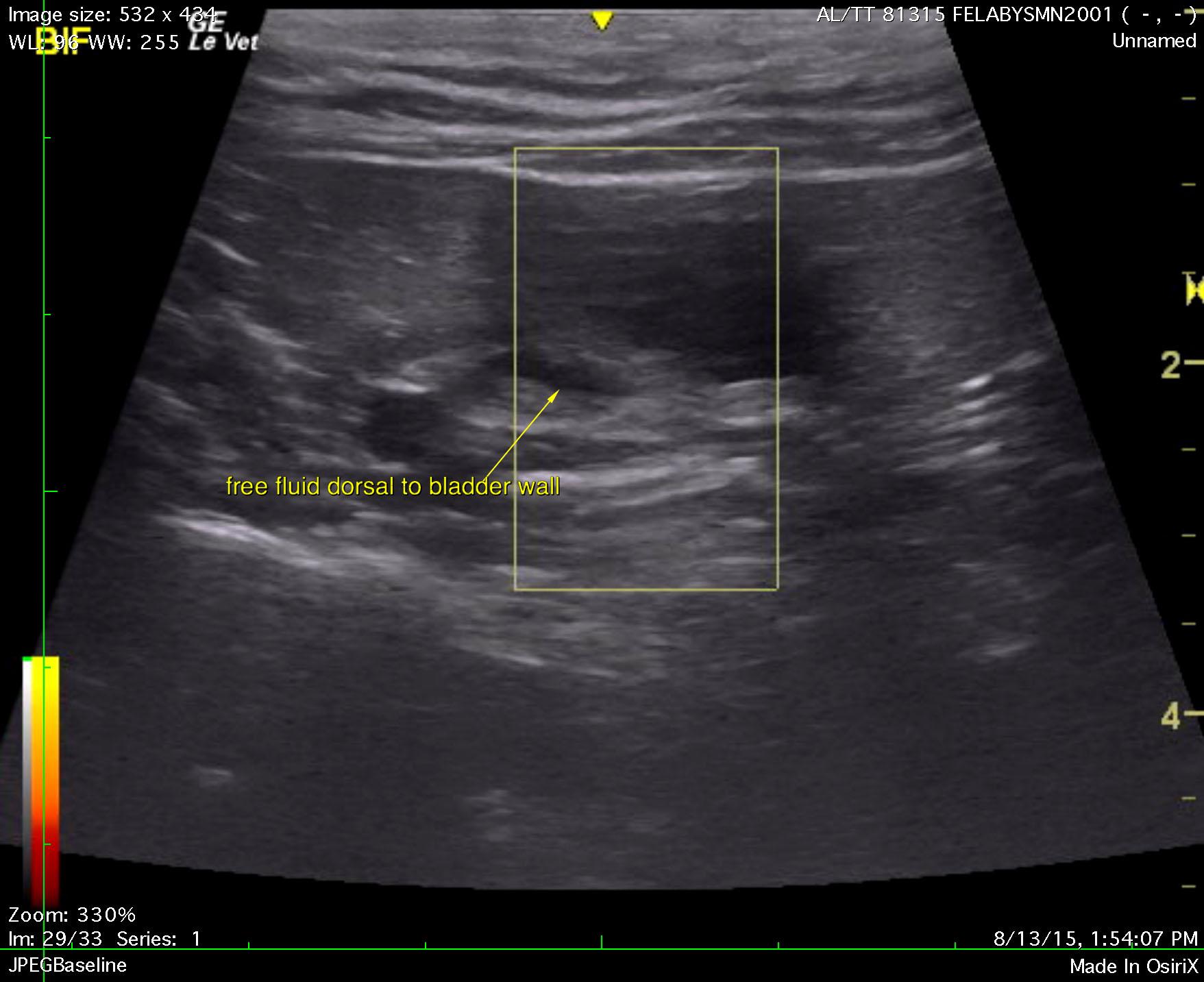
Chronic cystitis bladder pattern, potential for bladder lymphoma or transitional cell carcinoma with free fluid owing to inflammation or potential early perforation.
Benign cystic nodule in the deep left liver. This is likely a biliary adenoma.
The urinary bladder presented chronic cystitis pattern with excessive thickening. A minimal amount of urine was noted and the wall measured 0.82 cm. There is a potential for bladder lymphoma. Traumatic catheterization is recommended with cytology. The pelvic urethra was imaged 3.0 cm beyond the cystourethral junction and was structurally unremarkable. A trace amount of free fluid was noted craniodorsal to the bladder. Therefore, this is somewhat of a surgical urgency.
The kidneys presented an interstitial nephrosis pattern with minor irregular contour and microinfarcts. The right kidney measured 4.2 cm. The left kidney measured 3.0 cm.
Review of the bladder after filling revealed more of a chronic cystitis pattern with significant apical dorsal thickening. This may prove to be resectable. Power Doppler assessment of the wall appeared to be excessive. Periserosal inflammatory pattern was noted. Resection of the bladder would entail removal of approximately 2/3 of the cranial bladder. Guarded prognosis depending upon underlying cytology.