The patient is a 3 year old M canine mixed dog with grade I/V left pelvic limb lameness
The patient is a 3 year old M canine mixed dog with grade I/V left pelvic limb lameness
The patient is a 3 year old M canine mixed dog with grade I/V left pelvic limb lameness
The patient is a 3 year old M canine mixed dog with grade I/V left pelvic limb lameness
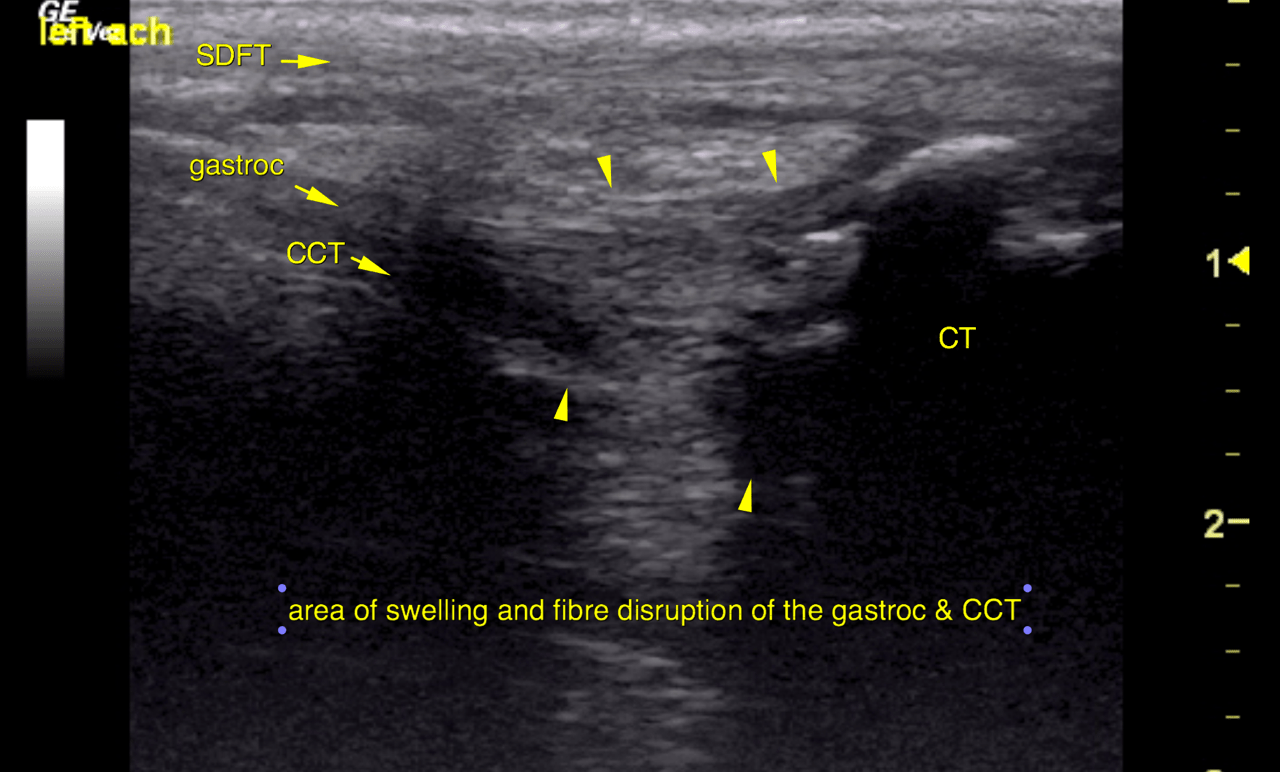
Ultrasound of the left calcanea region: Left:
Marked localized swelling with partial fibre disruption and decreased echogenicity is
noted for the gastrocnemius and common calcaneal tendons next to their calcaneal
insertion. The affected region spans approximately 1.5 cm immediately next to the
calcaneal tubercle.
The bone surface of the calcaneal tubercle presents marked irregularity and modeling
with concave defects and multiple protruding new bone formations.
The calcaneal bursa reveals enlargement, effusion and wall thickening. A moderate
amount of anechoic fluid is seen between the tendinous components on the calcaneal
tendon localized to the area of fibre disruption.
Irregular echogenic tissue proliferation is noted emphasizing the space between the
superficial digital flexor tendon (SDFT) and gastrocnemius tendon.
The SDFT presents no abnormalities.
The right calcaneal region was scanned for comparison and reveals no abnormalities.
The ultrasonographic findings are compatible with partial rupture of the deep
components of the calcaneal tendon (gastrocnemius and common calcaneal tendon)
with chronic bony modeling of the calcaneal tubercle. Biomechanical failure is likely
to develop.
Chronic bursitis and reactive tissue proliferation are noted as additional findings.
A traumatic origin with avulsion fracture possibly before reaching skeletal maturity is
most likely here. Degeneration with repetitive microruptures – such as in Doberman- is
a possible differential diagnosis but lower for potential since the disease appears to be
strictly unilateral and occurred at a young age whereas the degeneration usually occurs
bilaterally in dogs of medium age and presents with typical toe tipping stance & gait at
the point of biomechanical failure.
At this relatively advanced stage response to conservative management is questionable.
Successful healing is likely to require temporary fixation