Maverick is a 7 1/2 year old Lab with 2 fairly large cutaneous mast cell tumors.
On x-rays the spleen was prominent but not overly enlarged.
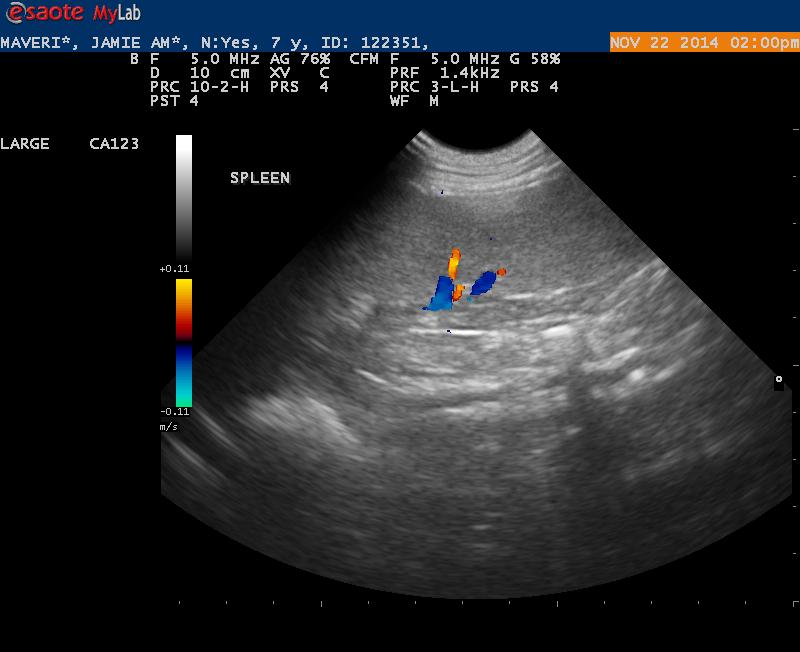
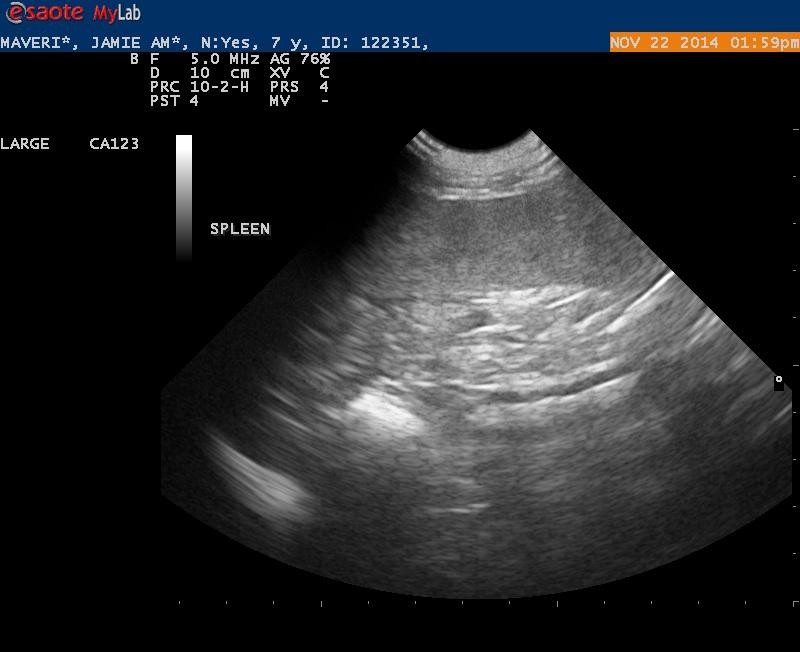
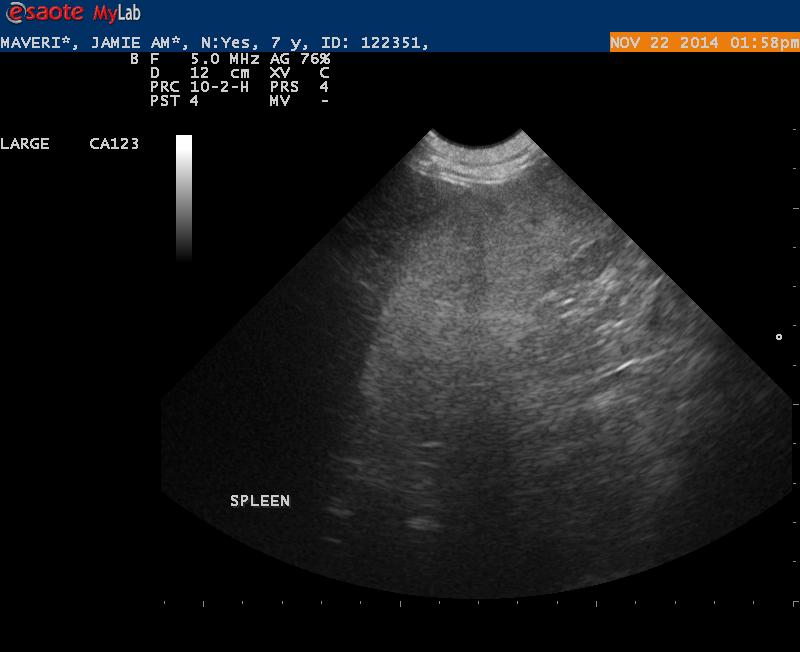
Ultrasound findings were within normal limits. I did not appreciate any lymphadenopathy.
The spleen on first glance appeared to be normal- but when I went back and looked at my images I was wondering if the echotexture was a bit coarse.
My questions for all that want to comment:
1. Do you see any abnormalities with this spleen making it worthwhile to get an aspirate?
Maverick is a 7 1/2 year old Lab with 2 fairly large cutaneous mast cell tumors.
On x-rays the spleen was prominent but not overly enlarged.
Ultrasound findings were within normal limits. I did not appreciate any lymphadenopathy.
The spleen on first glance appeared to be normal- but when I went back and looked at my images I was wondering if the echotexture was a bit coarse.
My questions for all that want to comment:
1. Do you see any abnormalities with this spleen making it worthwhile to get an aspirate?
2. Do you routinely aspirate spleen or liver even if they appear to be grossly normal?
Thanks

6 responses to “MCT”
Not obvious age related
Not obvious age related spleen mainly with minor heterogenous changes but if any doubt 25 g fna is always a good idea with mct
Not obvious age related
Not obvious age related spleen mainly with minor heterogenous changes but if any doubt 25 g fna is always a good idea with mct
Recent publication:
Warland
Recent publication:
Warland J, Amores-Fuster I , Newbury W, Brearley M, Dobson J. The utility of staging in canine mast cell tumours. Veterinary and Comparative Oncology. 2014; 12: 287–298
Current staging of canine mast cell tumours (MCTs) practiced by many veterinarians involves a minimum of lymph node (LN) assessment, abdominal ultrasound and thoracic radiography. Historically, some have advocated buffy coat and bone marrow evaluation. Two hundred and twenty dogs with MCT seen at a referral clinic were staged using LN palpation/cytology, thoracic radiography and abdominal ultrasound. The utility of each method was evaluated by considering prevalence of spread and future behaviour. At presentation, 30.9% of dogs had metastases to the local LN; 6.8% of all the dogs also had distant metastases. No dog had or developed distant metastasis in the absence of LN metastasis. No dog had convincing evidence of pulmonary metastasis. In this series, the local LN was sentinel to metastasis and in the absence of local LN metastasis; the utility of further staging was low. Thoracic radiography was not useful in the staging of canine MCT.
Recent publication:
Warland
Recent publication:
Warland J, Amores-Fuster I , Newbury W, Brearley M, Dobson J. The utility of staging in canine mast cell tumours. Veterinary and Comparative Oncology. 2014; 12: 287–298
Current staging of canine mast cell tumours (MCTs) practiced by many veterinarians involves a minimum of lymph node (LN) assessment, abdominal ultrasound and thoracic radiography. Historically, some have advocated buffy coat and bone marrow evaluation. Two hundred and twenty dogs with MCT seen at a referral clinic were staged using LN palpation/cytology, thoracic radiography and abdominal ultrasound. The utility of each method was evaluated by considering prevalence of spread and future behaviour. At presentation, 30.9% of dogs had metastases to the local LN; 6.8% of all the dogs also had distant metastases. No dog had or developed distant metastasis in the absence of LN metastasis. No dog had convincing evidence of pulmonary metastasis. In this series, the local LN was sentinel to metastasis and in the absence of local LN metastasis; the utility of further staging was low. Thoracic radiography was not useful in the staging of canine MCT.
Awesome thanks remo!
Awesome thanks remo!
Awesome thanks remo!
Awesome thanks remo!