A 15-year-old MN DSH that had been diagnosed with diabetes and renal disease was presented for evaluation. Current therapy was glargine BID. The only abnormality on serum biochemistry was azotemia (creatinine 2.5, BUN 21). Glucose was within reference range (glucose122).
A 15-year-old MN DSH that had been diagnosed with diabetes and renal disease was presented for evaluation. Current therapy was glargine BID. The only abnormality on serum biochemistry was azotemia (creatinine 2.5, BUN 21). Glucose was within reference range (glucose122).
Chronic kidney disease, renoliths, pyelonephritis, obstructive uropathy, hypertensive nephropathy, diabetic nephropathy.
Stable diabetic
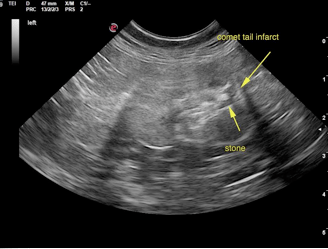
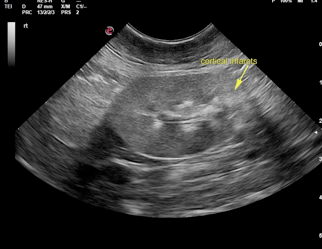
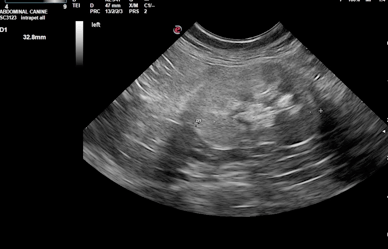
The kidneys presented cortical infarcts and remodeling. The left kidney revealed a comet tail infarct in the caudal pole. Slight pyelectasia was noted. The kidneys otherwise revealed a chronic interstitial nephrosis pattern. Kidney changes are likely owing to acute on chronic disease owing to variable infarcts and stone movement with potential concurrent infection. The right kidney measured 3.66 cm. The left kidney measured 3.28 cm.
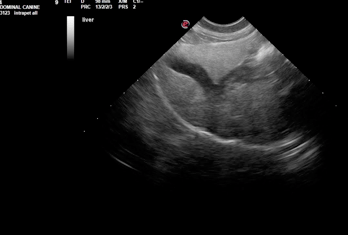
The hepatic parenchyma was uniformly hyperechoic without disruption of architecture. No masses were noted. The gall bladder and common bile duct were unremarkable. This presentation is most consistent with hepatic lipidosis of variable degree with the minor potentially for underlying lymphoma or inflammatory hepatopathy that is not structurally evident at this time. The potential for these latter pathologies would be based on hepatic enzyme elevations and clinical profile. US-guided FNA s warranted if any elevation in SAP or bilirubin in is present or if anorexia is present to assess cytological disease (lipidosis or round cell neoplasia). Biopsy is warranted if an elevation in ALT is present to assess hepatic portal instrastructure.