This 15 year old MN Burmese cat has a history of brachycephalic airway syndrome and hyperthyroidism, both controlled. Currently vomiting soon after eating; decreased appetite. IRIS stage 2 CKD, stable
Physical exam: congested upper airway with audible and palpable bubbles over cervical trachea and severe stenotic nares.
This 15 year old MN Burmese cat has a history of brachycephalic airway syndrome and hyperthyroidism, both controlled. Currently vomiting soon after eating; decreased appetite. IRIS stage 2 CKD, stable
Physical exam: congested upper airway with audible and palpable bubbles over cervical trachea and severe stenotic nares.
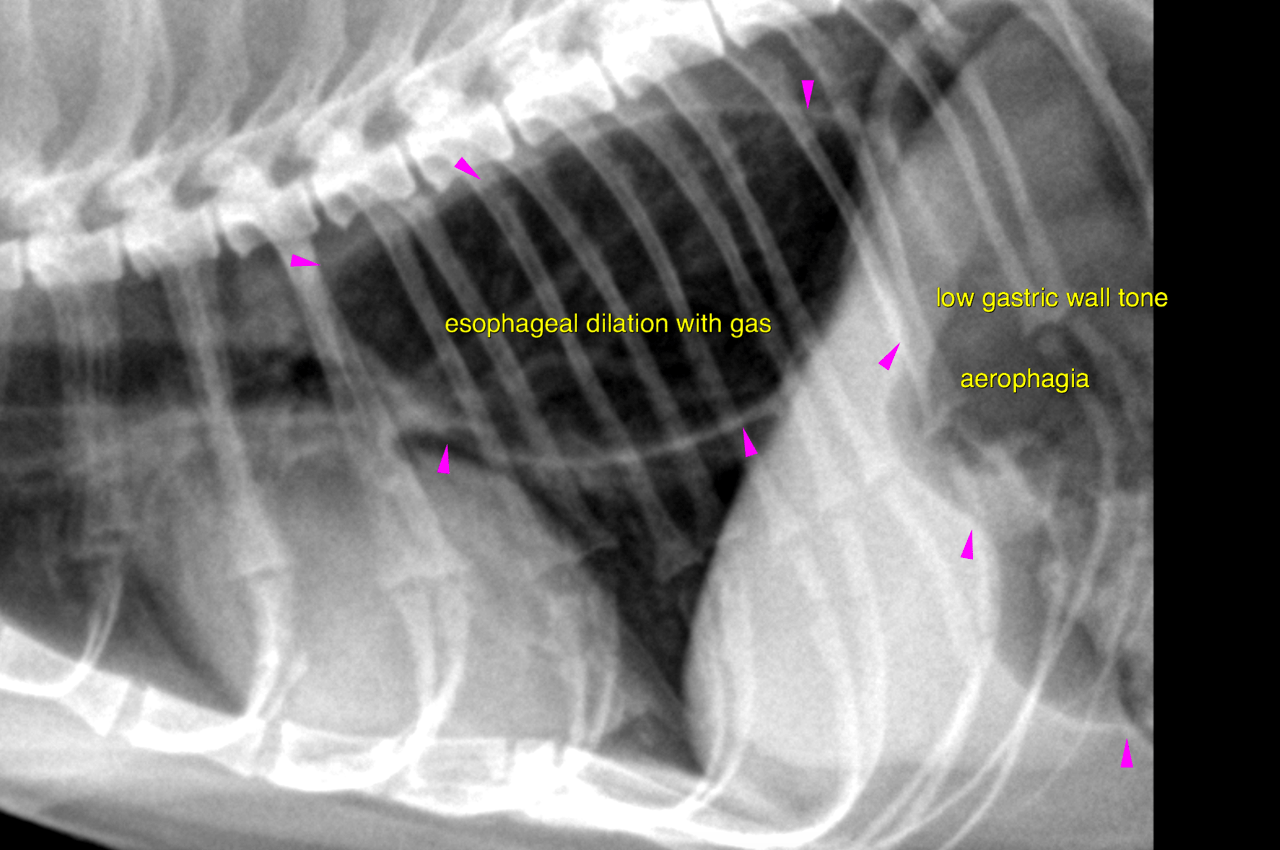
• Megaesophagus; gastric dysmotility; No evidence of aspiration pneumonia; Possible compensated thyrotoxic/hypertensive cardiomyopathy without evidence of congestive failure
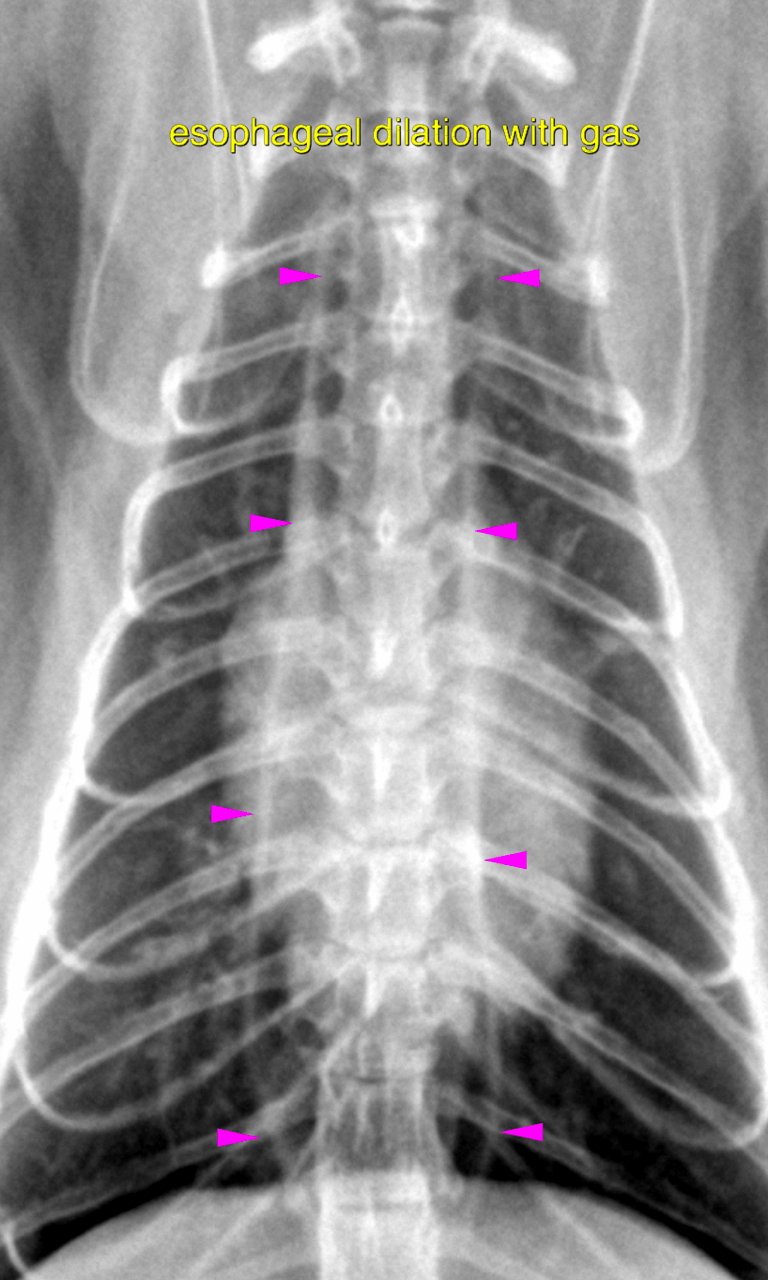
lateral and vd thorax – There is no evidence of an
abnormal pulmonary infiltrate throughout the lungs.
Moderate generalized dilation of the intrathoracic esophagus with gas is noted. The
stomach is moderately distended with gas. The gastric wall tone appears to be low.
Several incomplete contraction waves appear to pass through the gastric fundus and
body.
Possible underlying causes include idiopathic, neuromuscular disease (myasthenia
gravis, feline dysautonomia, polymyositis, polyneuropathy), autoimmune,
paraneoplastic, esophagitis, endocrine (hypoadrenocorticism), electrolyte disturbances,
toxicity (lead, thallium).
The simultaneous presence of esophageal and gastric motility disorder makes a
neuromuscular disease more likely than the other causes. Radiographically there is no
evidence of an esophageal forein body, neoplasia or other source of obstruction to be
the underlying issue here. Next to bloodwork full workup may require Acetylcholine antibody testing,
neuromuscular biopsy as well as esophagoscopy.