An 8-year-old NM Labrador Retriever with a history of seizures, cardiac disease, and pacemaker implantation was presented for evaluation of decreased appetite and progressive azotemia. Current therapy was enalapril, phenobarbital and potassium bromide.
An 8-year-old NM Labrador Retriever with a history of seizures, cardiac disease, and pacemaker implantation was presented for evaluation of decreased appetite and progressive azotemia. Current therapy was enalapril, phenobarbital and potassium bromide.
Renal – chronic kidney disease, pyelonephritis, bacterial nephritis, infarction, neoplasia, renoliths
Addison’s disease
Progressive cardiac disease
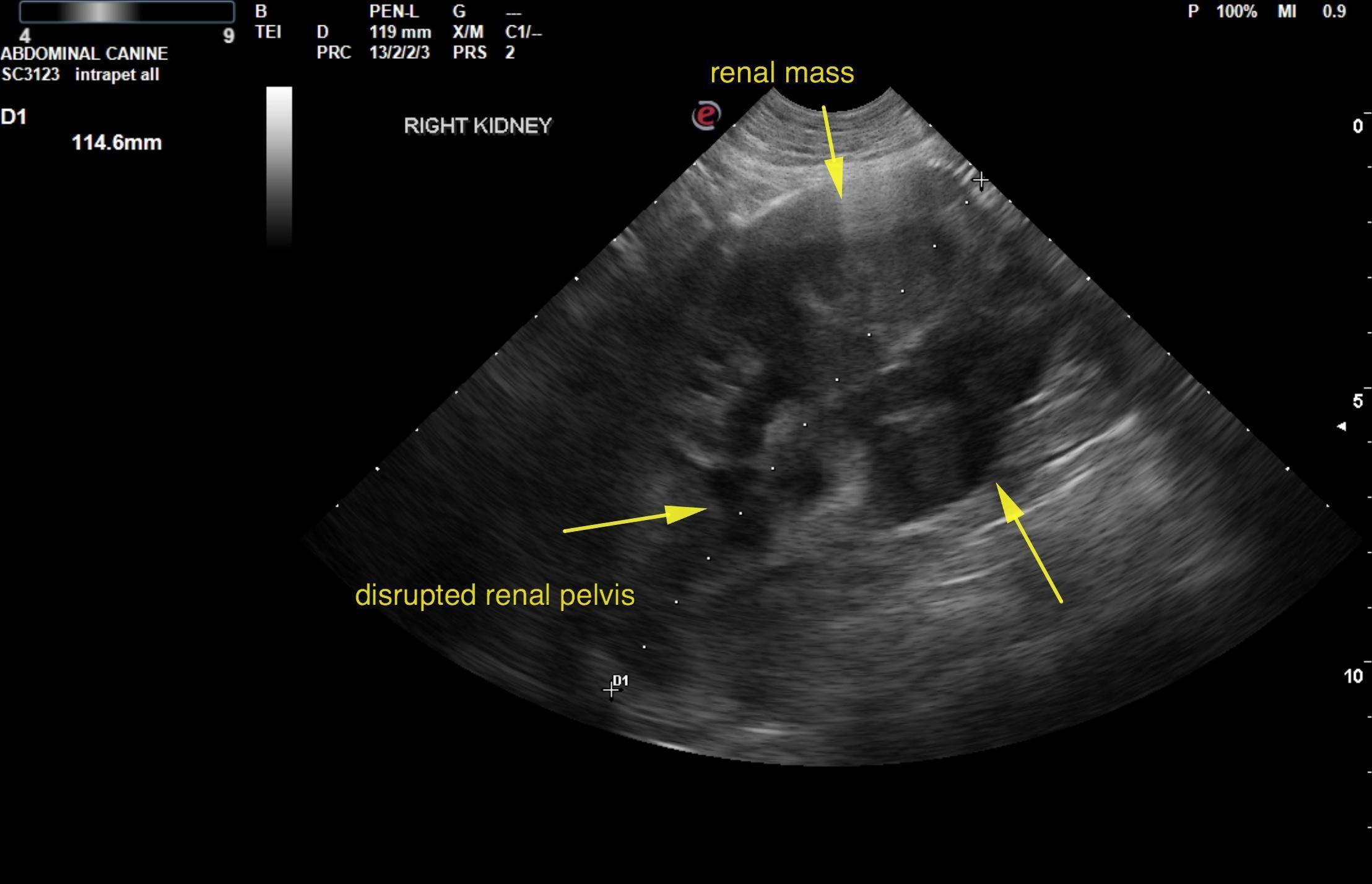
Right renal mass. Age related renal, hepatic changes or potential early multi focal neoplasia.
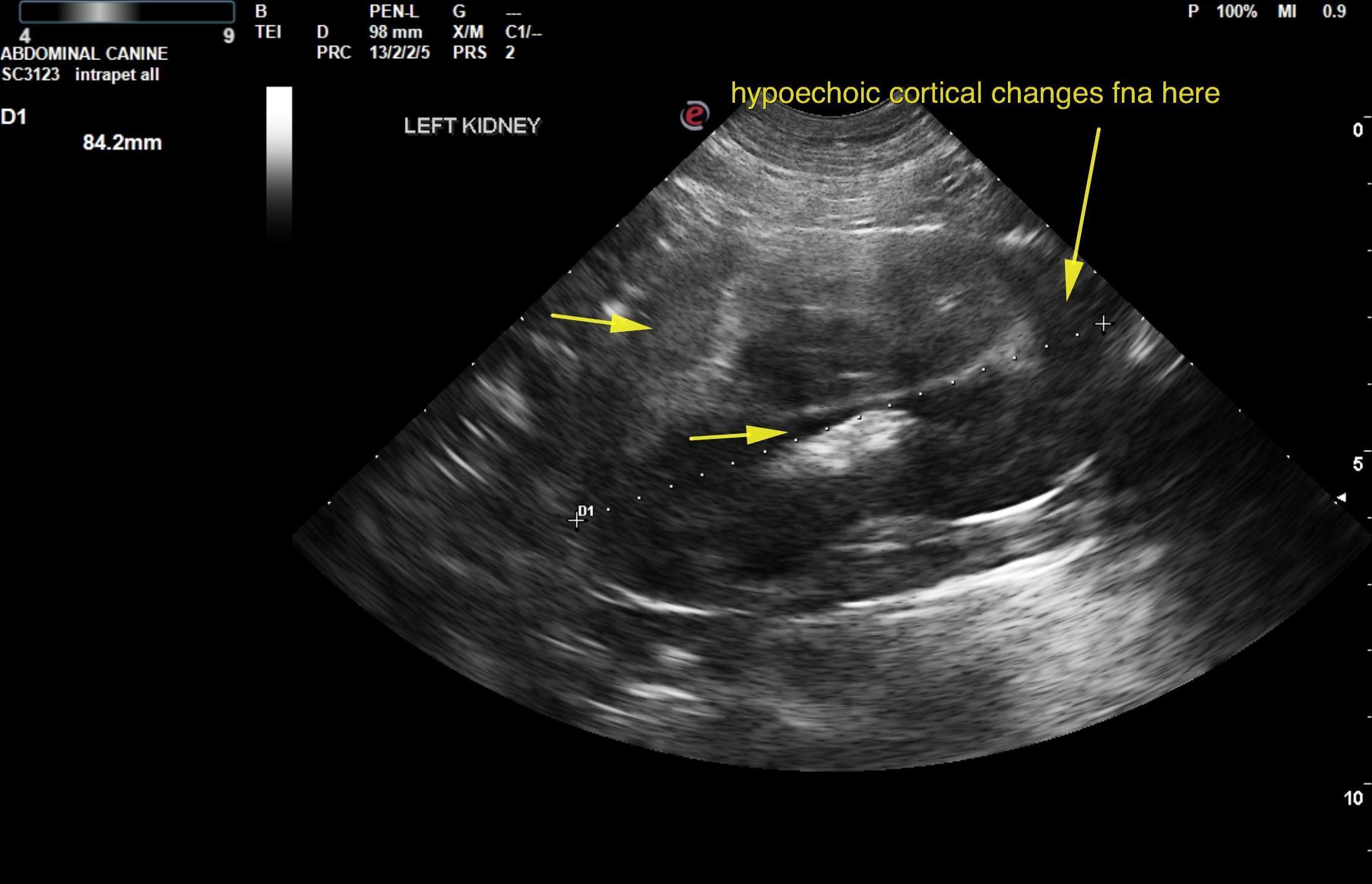
The right kidney in this patient presented an expansive, nodular, hypoechoic mass. This is strongly suggestive for round cell neoplasia. Complete disruption of the renal pelvis was noted. The right kidney measured 11.4 cm. The left kidney presented minor pyelectasia with slight heterogenous, hypoechoic cortical changes. Ultrasound-guided FNA is recommended to assess if an early infiltrative process is present. While the right kidney is completely distorted with pericapsular inflammatory pattern, the left kidney presents largely age related changes with subtle, hypoechoic cortical changes that may represent an early metastatic disease. Slight, retroperitoneal fluid was noted around the right kidney.
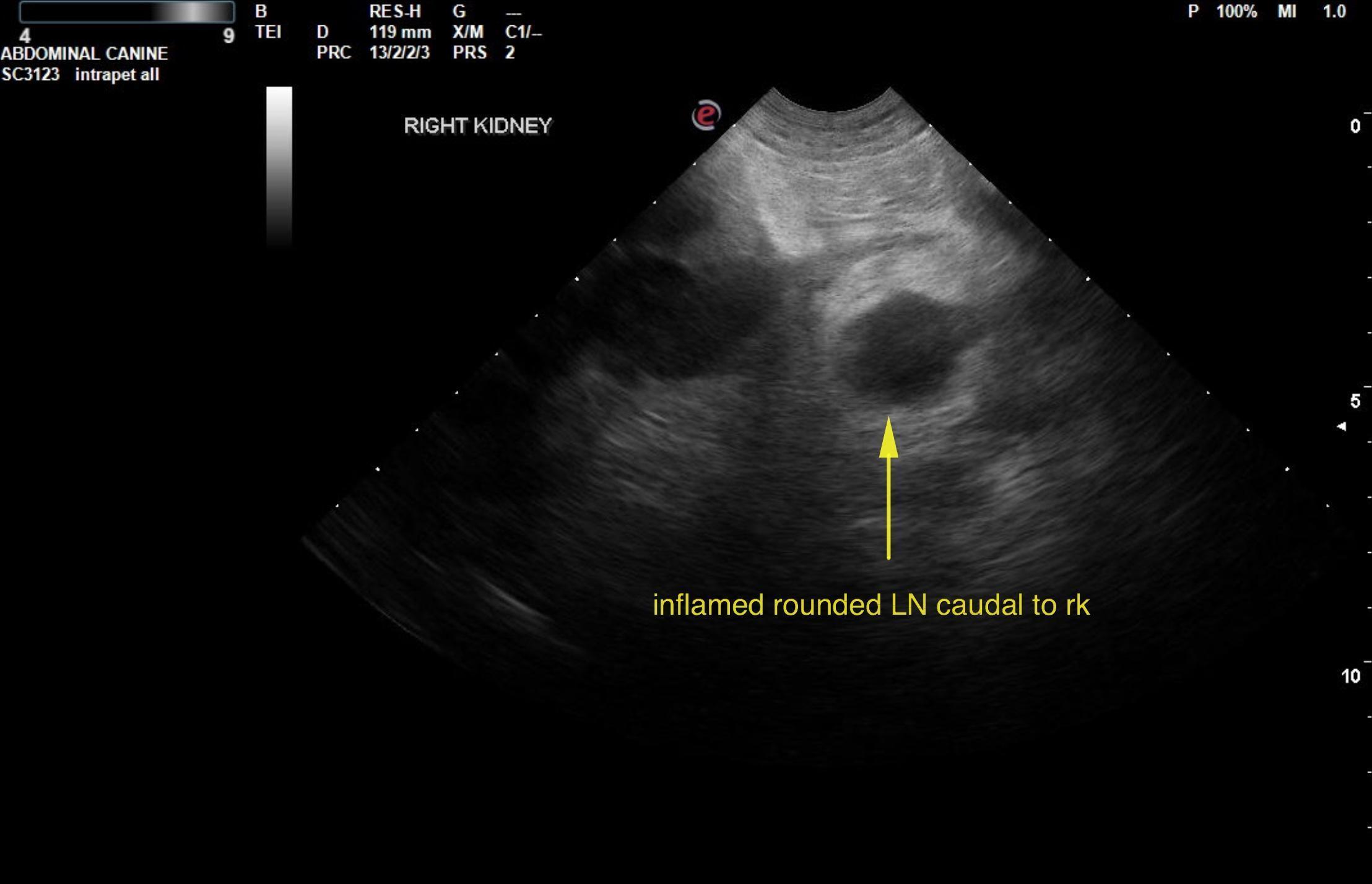
A 2.0 cm, hypoechoic, rounded infiltrated lymph node with pericapsular inflammatory pattern was noted caudal to the right kidney. This is strongly suggestive for local spread. Removal at surgery could be considered.
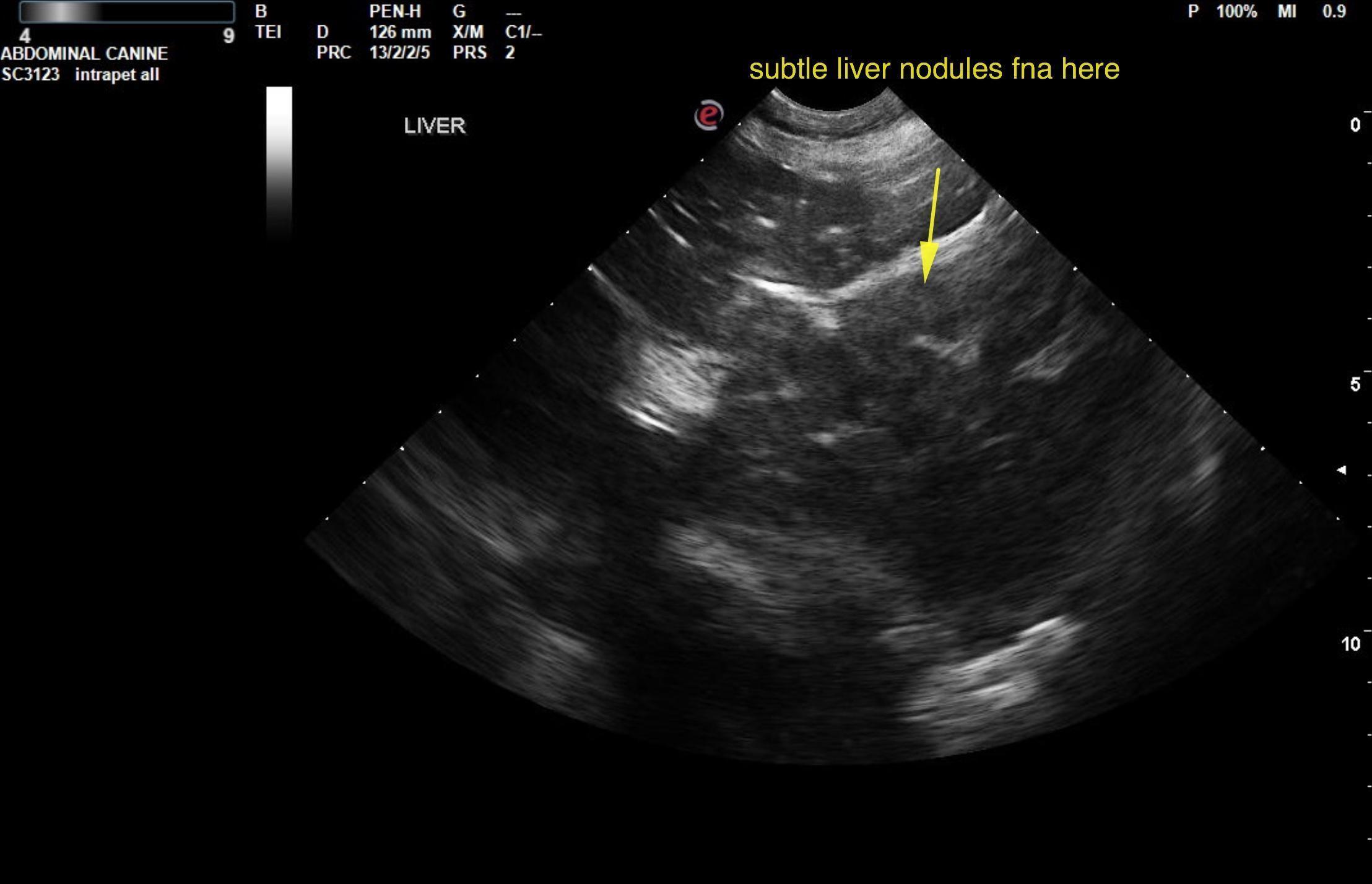
screening process of FNA of the left kidney cortex, liver and right kidney is recommended to define the neoplastic process in the right kidney and assess if metastatic disease is present elsewhere. If the left kidney and liver are clean and there is no evidence of neoplasia then right nephrectomy is warranted as long as three view chest radiographs and cranial mediastinum/sternal lymph nodes are not involved. Guarded prognosis. Chemotherapy will be necessary. Round cell neoplasia versus renal carcinoma are the primary differentials. Removal of the lymph node at the time of surgery could be considered or direct chemotherapy based on aspirate results. FNA of the lymph node would also be ideal.