The Restrictive Cardiomyopathy Cat, a Saddle Thrombus, & Today’s Cutting Edge Effective Pharmacy.
Yes the kitchen sink of medications were necessary to pull this cardiomyopathy cat through a saddle thrombus. Plavix, pimobendan, ace-inhibitor, atenolol, lasix, heat support and whatever else came to mind….A fortunate 21st century cat and excellent care prevailed thanks to a trio of local intensive care, mobile sonography, and remote cardiology consultation. You have to love where we are in the “Flat” veterinary world of 2012.
The Restrictive Cardiomyopathy Cat, a Saddle Thrombus, & Today’s Cutting Edge Effective Pharmacy.
Yes the kitchen sink of medications were necessary to pull this cardiomyopathy cat through a saddle thrombus. Plavix, pimobendan, ace-inhibitor, atenolol, lasix, heat support and whatever else came to mind….A fortunate 21st century cat and excellent care prevailed thanks to a trio of local intensive care, mobile sonography, and remote cardiology consultation. You have to love where we are in the “Flat” veterinary world of 2012.
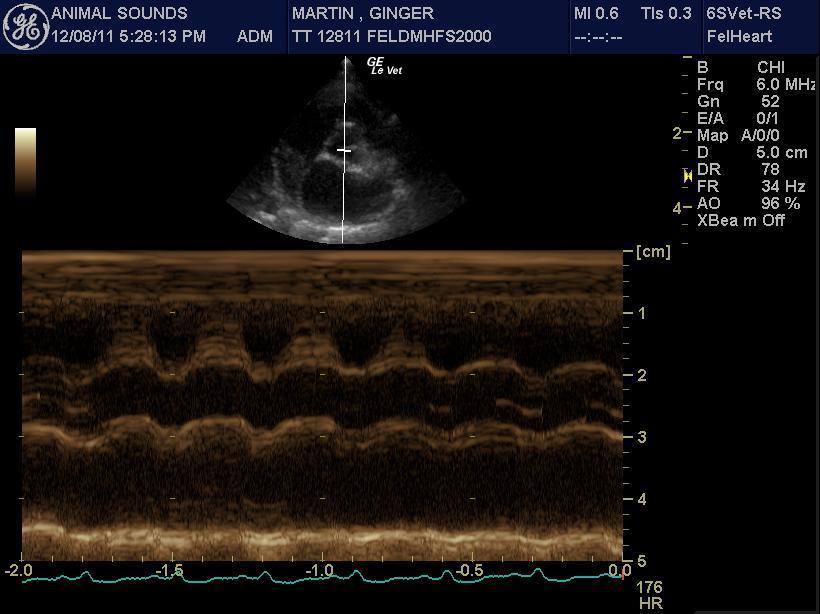
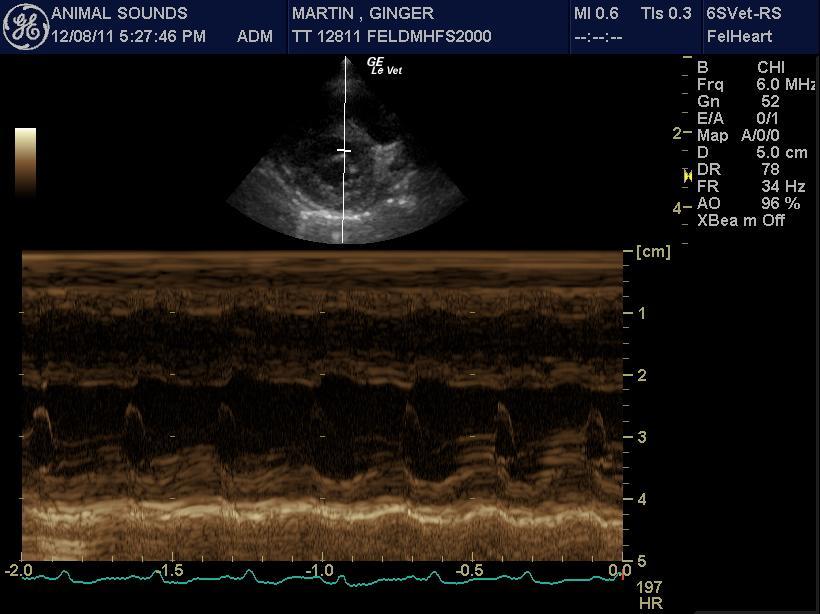
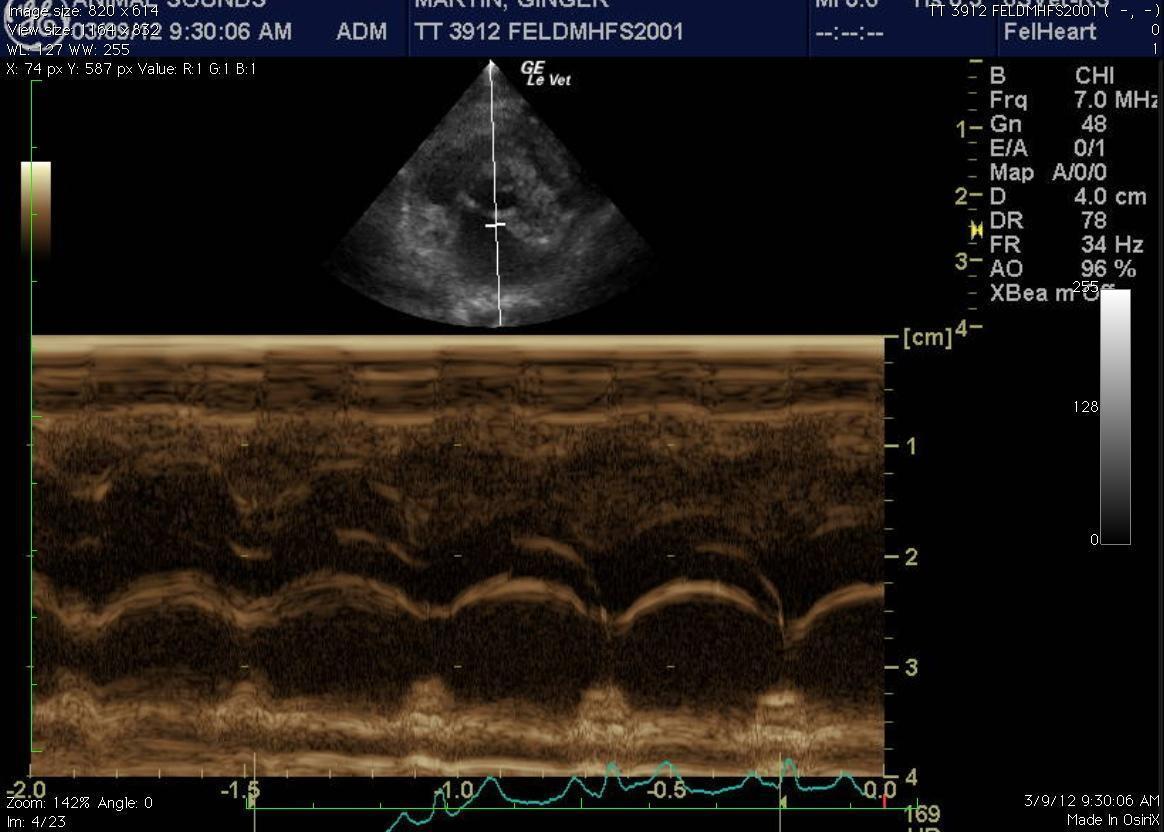
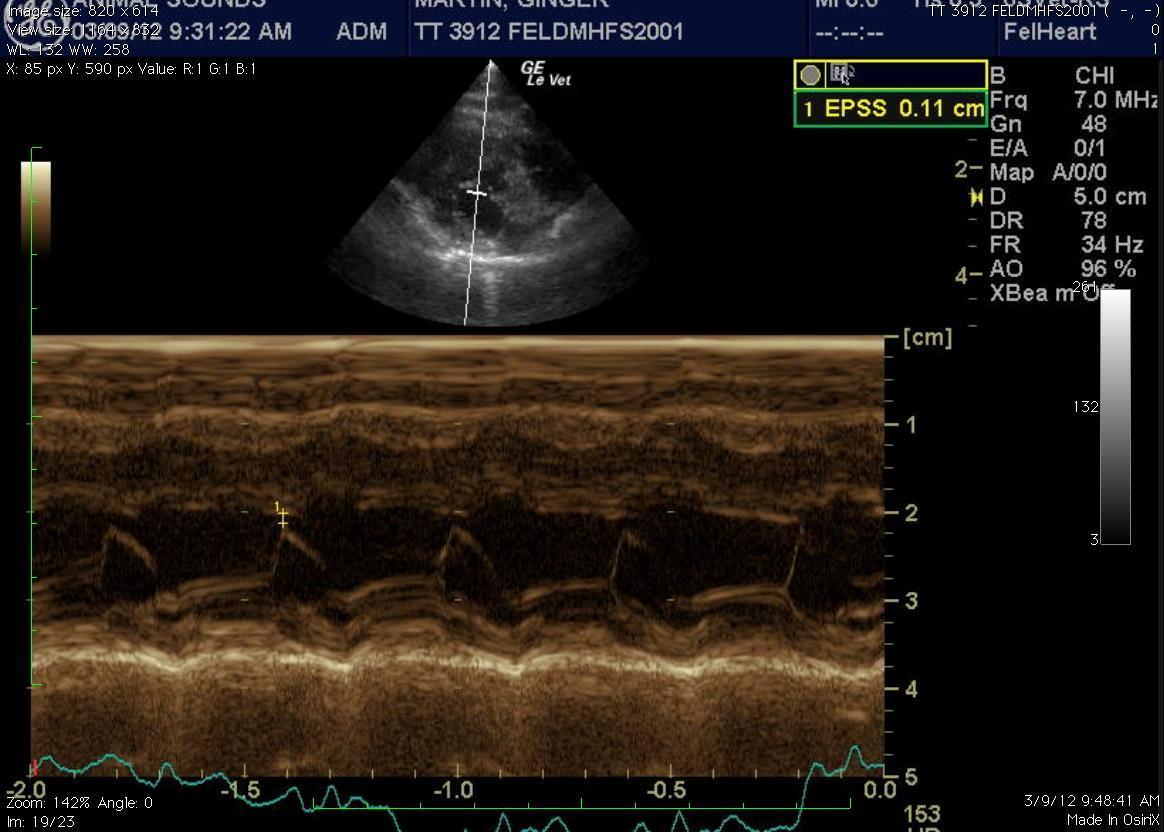
Sonogram (Cardiac): Ginger Martin
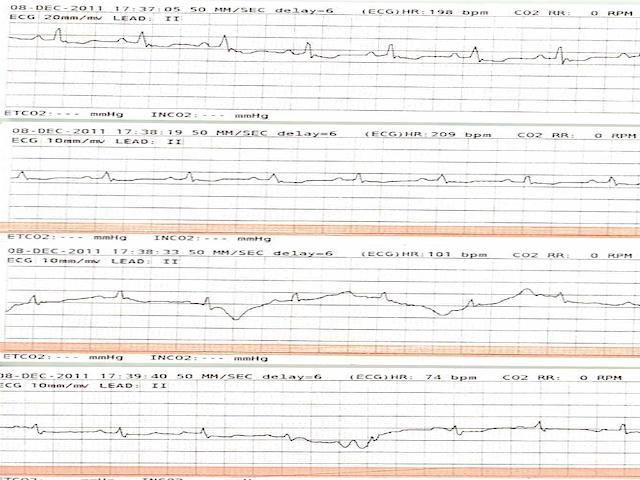
History: The patient is a feline DMH, SF, 9 year old. The patient has a history of hyperthyroidism, treated with I 131, sudden onset posterior paresis. The physical exam revealed poor femoral pulse quality, knuckling of hind limbs, gallop rhythm, and hypothermia (97.2 F). The patient was able to move the rear paws but could not stand. Bloodwork revealed slight hyperglycemia, moderate anemia, polychromasia and anysicytosis. Thrombocytopenia with clumping was also noted.
(Remo Lobetti PhD, DECVIM):
Saddle thrombosis secondary to cardiac disease – dilated cardiomyopathy, hypertrophic cardiomyopathy, restrictive cardiomyopathy
Spinal – trauma, disc, neoplasia
Myopathy – trauma, infectious
(J. Betkowski DVM, DACVIM Cardiology): Heparin can be considered at 200 U/kg IV once followed by 100 U/kg SQ QID while the cat is hospitalized. Other supportive care such as pain medications can be considered as clinically warranted. Low dose Lasix such as 6.25 to 7.5 mg IV q 12 to 24 hours can be considered, particularly if the respiratory rate were elevated. This can be continued as a maintenance therapy, perhaps at 6.25 mg PO SID or whatever is the lowest dose that will control the clinical signs. Pimobendan is also recommended at 0.625 to 1.25 mg PO BID. Once the cat has improved, Benazepril can be added at 1.25 mg PO SID and increased to 2.5 mg PO SID after a week if it is well tolerated. If the heart rate were persistently elevated over 180 bpm, Atenolol would be recommended at 1/4 of a 25 mg tablet PO SID to BID to keep the heart rate in the normal range. Long-term anti-coagulation can be considered with aspirin or Ascriptin at 5 mg/kg or 5 mg total dose PO on a Monday, Wednesday, Friday schedule with Plavix at ¼ of a 75 mg tablet PO SID. A renal profile is recommended a week after the final adjustments to the medications have been made to make sure they are well tolerated. The condition can be followed by thoracic radiographs every 2 to 5 months to monitor for signs of progression or decompensation. The echocardiogram can be repeated in 6 months to monitor for any further changes to the cardiac structure.