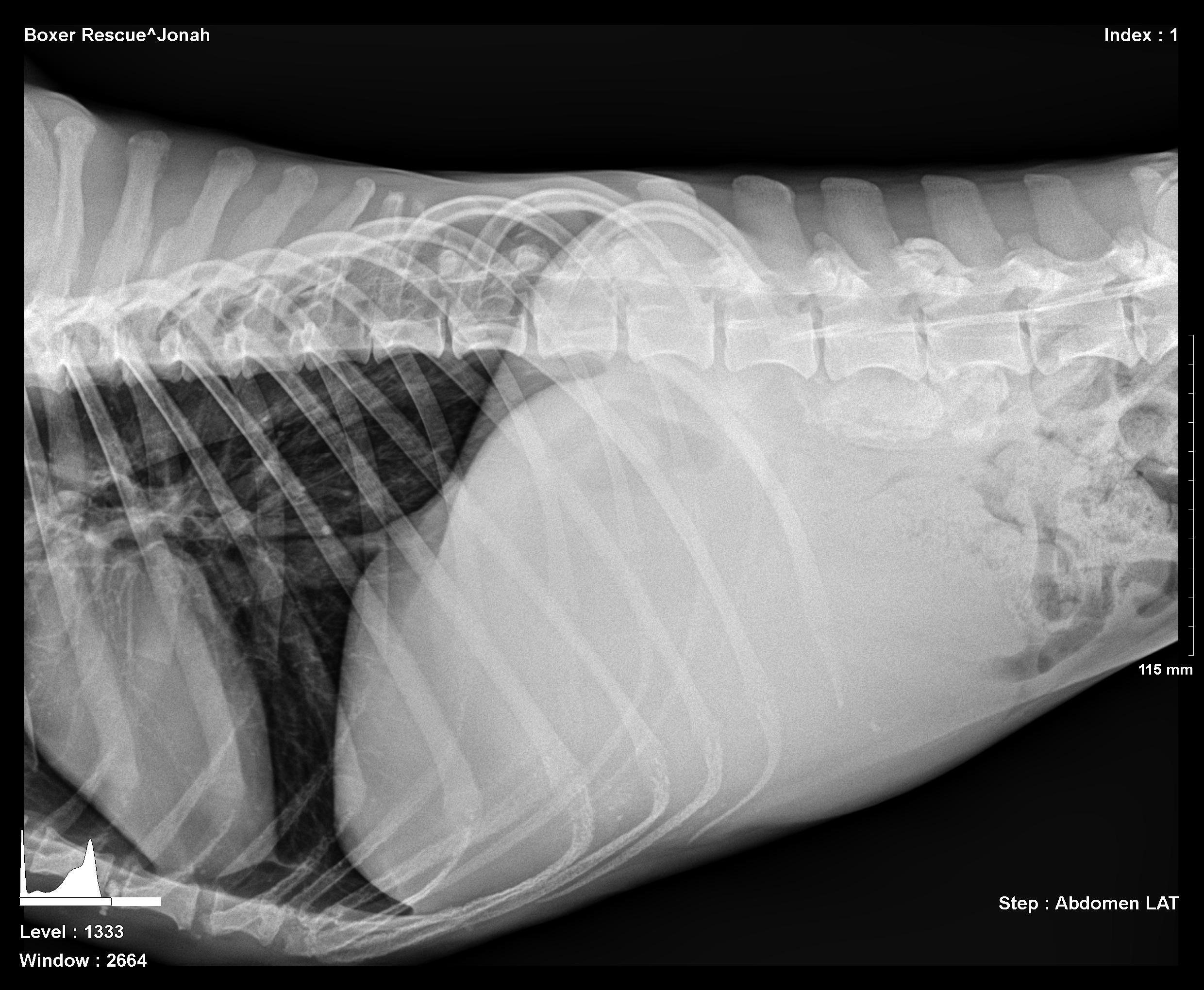
The patient is a canine Boxer, NM, 5 years of age presented to the clinic by a rescue organization. The patient was emaciated, vomiting and anorexic. Bloodwork was unremarkable. Physical exam revealed a mid abdominal thickening potentially of intestinal origin. Lateral radiograph revealed a mid cranial abdominal mass with mass effect upon the intestinal tract displacing the mesentery caudally. A volume-contracted heart was also visible. Image 1.
The patient is a canine Boxer, NM, 5 years of age presented to the clinic by a rescue organization. The patient was emaciated, vomiting and anorexic. Bloodwork was unremarkable. Physical exam revealed a mid abdominal thickening potentially of intestinal origin. Lateral radiograph revealed a mid cranial abdominal mass with mass effect upon the intestinal tract displacing the mesentery caudally. A volume-contracted heart was also visible. Image 1.
GI tract – neoplasia, foreign body, IBD
Pancreas – chronic pancreatitis, neoplasia
Abdominal mass – neoplasia/cyst/granuloma of intestine, spleen, liver.
(http://www.sonopath.com/about/specialists/remo-lobetti)
Obstructive foreign body with likely underlying mural disease and minor regional omental inflammation.
Exploratory surgery with enterotomy, gastric and intestinal biopsies were recommended. Guarded prognosis depending on underlying histopathology whether concurrent intestinal neoplasia is present versus inflammatory related mural hypertrophy.
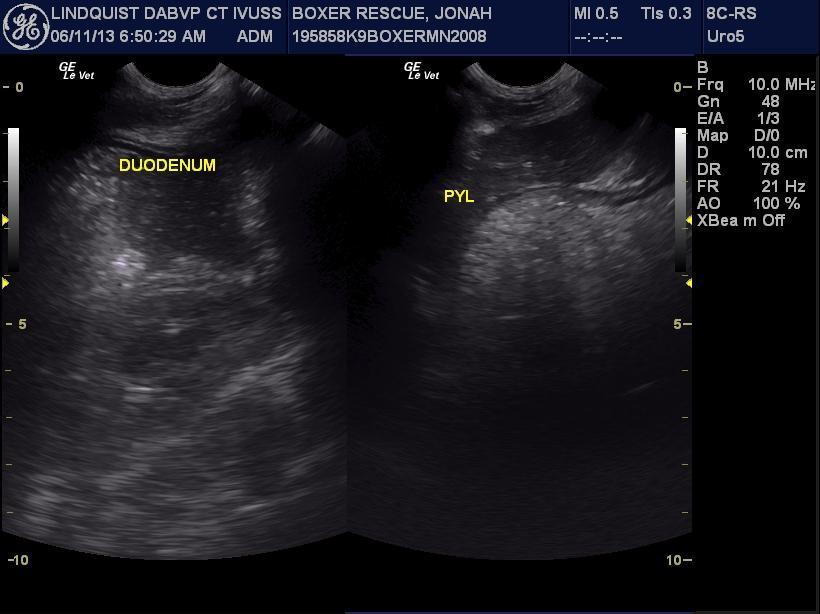
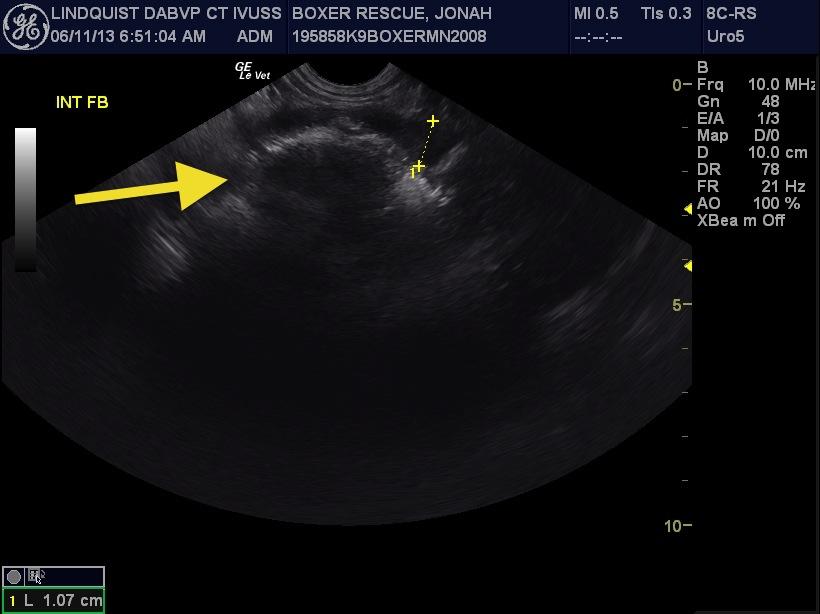
Image 2: Split screen of stomach (right) and duodenum (left) that revealed upper GI stasis. Image 3: A distinctly shadowing intestinal foreign body is seen (arrow) with mural thickening and loss of layering of the affected intestinal wall (measurement). Images 4 & 5: The 6 cm shadowing foreign body is visible with adjacent stasis followed by empty small intestine finalizing the obstructive pattern defined in our prior study (Sonographic Criteria for the Diagnosis of Gastrointestinal Obstruction in 39 Dogs and Cats, ECVIM 2009, http://www.sonopath.com/resources/articles). A minor amount of ill-defined surrounding fat is noted adjacent to the intestinal wall in the near field indicative of transmural disease process in act indicating a surgical emergency before further breakdown of the intestinal wall occurs.