Where the heck is the azygos vein and what shunt goes there? You can diagnose a shunt on a sonogram. Sure, with practice and the right technique you can and we love to do it here in the SonoPath community….it’s geeky fun for us with tons of U/S shunt examples in our clinical search engine (http://www.sonopath.com/clinical-search-and-pathology-search) and more are in past cases of the month in the resources tab (http://www.sonopath.com/resources).
Also see our abstract on the subject in sonopath resources: (http://www.sonopath.com/resources/articles) ECVIM, Tolousse, France. Sept 8-11, 2010. Sonographic Whole Body Parameters of Portosystemic Shunts in 38 Dogs & Cats.
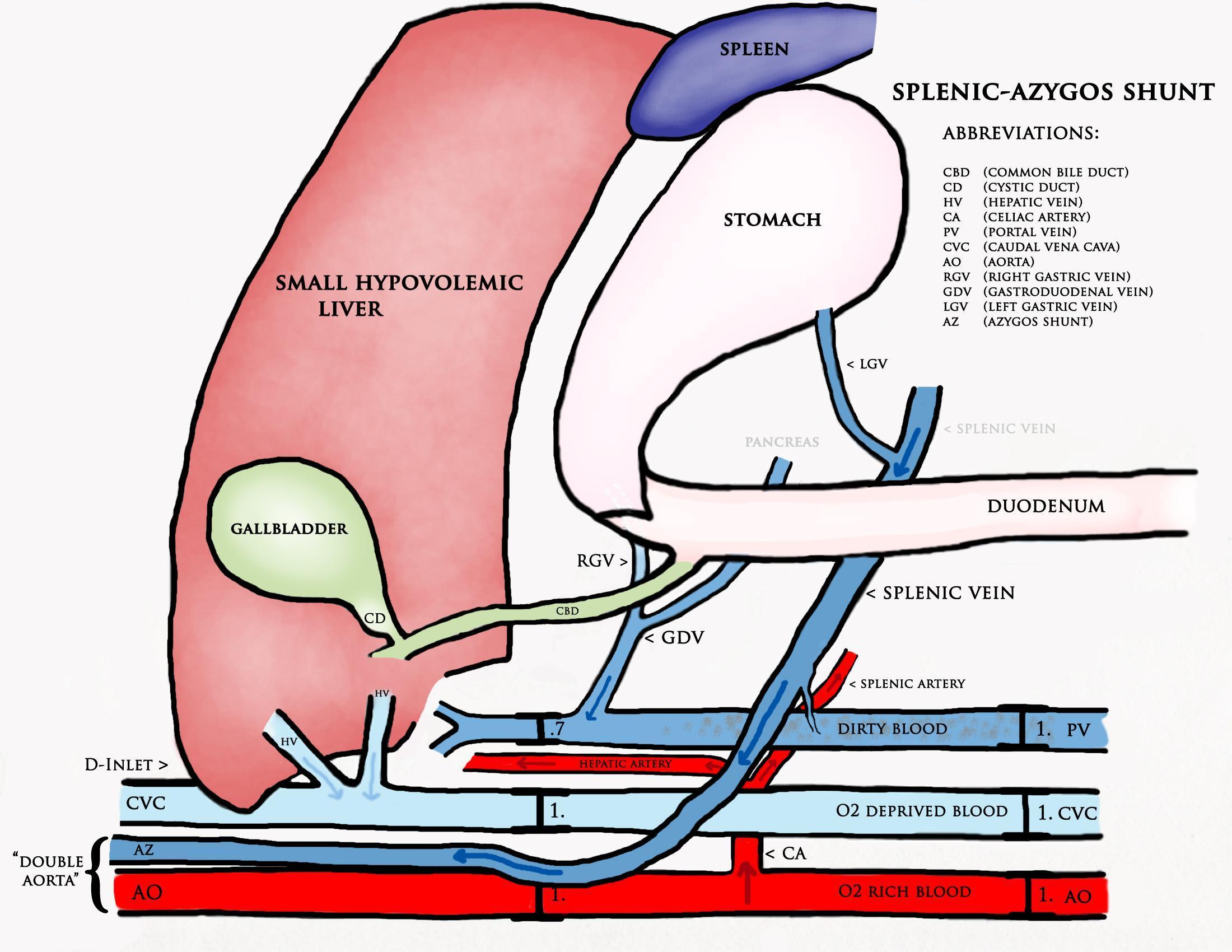
Well, the splenoazygos shunt, as we display here, can be found in Florida under the U/S probe of Seth Mitchell, DVM of Mobile Veterinary Imaging of SE Florida. (http://www.mobileveterinaryimaging.net/meet-our-team.html) Then what do we do with the shunt? Is the shunt surgical? Is it medical? We have criteria to tell the difference and Seth’s case is doing well on medical treatment alone after collaborating with SonoPath to ensure this challenging scenario. Come see how it shakes out in the December 2013 SonoPath case of the month (www.sonopath.com).
An 8-year-old FS Maltese was presented for evaluation for severely elevated pre and post-prandial bile acids and mild ALT elevations and subnormal BUN. In addition, the patient was positive for Rocky Mountain spotted fever. Seizure activity was present in the history.
An 8-year-old FS Maltese was presented for evaluation for severely elevated pre and post-prandial bile acids and mild ALT elevations and subnormal BUN. In addition, the patient was positive for Rocky Mountain spotted fever. Seizure activity was present in the history.
Porto-caval shunt, primary portal vein hypoplasia, hepatic fibrosis, liver cirrhosis. Primary CNS disease: inflammatory/infectious, neoplasia, GME.
Spleno-azygos shunt with chronic inflammatory hepatopathy.
The urinary bladder presented a small concretion that measured 0.5 cm and was non-shadowing. The kidneys presented a significant amount of pelvic mineralization that was non obstructive. The left kidney measured 3.6 cm. Calculus was noted in the left kidney pelvis and measured 1.16 cm. The right kidney measured 4.24 cm with pelvic calculus that measured 1.49 cm. The liver was subnormal in size with coarse architecture and increased portal markings. The vena cava measured 0.74 cm, aorta 0.62 cm. The portal vein was subnormal in size and measured 0.29 cm. An extrahepatic, portosystemic shunt was noted. This was deriving from the splenic vein entrance into the portal vein. This was tortuous and measured approximately 0.5 cm in width and traveled dorsally and entered into the aortic hiatus. This created a splenoazygos shunt and a “double aorta” was formed. Concurrent hepatic disease is likely given the increased portal markings and remodeling.