GB Mucocele: Its Not About The Kiwi! Thanks to the diagnostic efficiency workflows of Rebekah Jakum ARDMS of Pennsylvania Mobile Ultrasound (www.pamobile.net), Phil Zeltzman DVM, DACVS (www.drphilzeltzman.com), & Rossmoyne Animal Emergency (raetc.com) & yours truly (http://sonopath.com/about/specialists/eric-lindquist-dmv) to get this case from sonogram to interpretation to surgical table within a couple of hours so the bile peritonitis bomb that went off in this dog could be addressed immediately. Diagnostic efficiency in a nutshell represented by this month’s case of the month: Ruptured GB mucocele in Labrador with bland clinical profile.
12-year-old MN Labrador mixed breed was presented for evaluation of anorexia, vomiting, and lethargy. Abnormalities on CBC and serum biochemistry were severe leukocytosis,neutrophilia, hemococentration, and elevated ALP (600).
12-year-old MN Labrador mixed breed was presented for evaluation of anorexia, vomiting, and lethargy. Abnormalities on CBC and serum biochemistry were severe leukocytosis,neutrophilia, hemococentration, and elevated ALP (600).
Gallbladder – cholecystitis, mucocele, rupture. Liver- neoplasia, abscess. Pancreas- pancreatitis, neoplasia. Abdominal cavity- peritonitis.
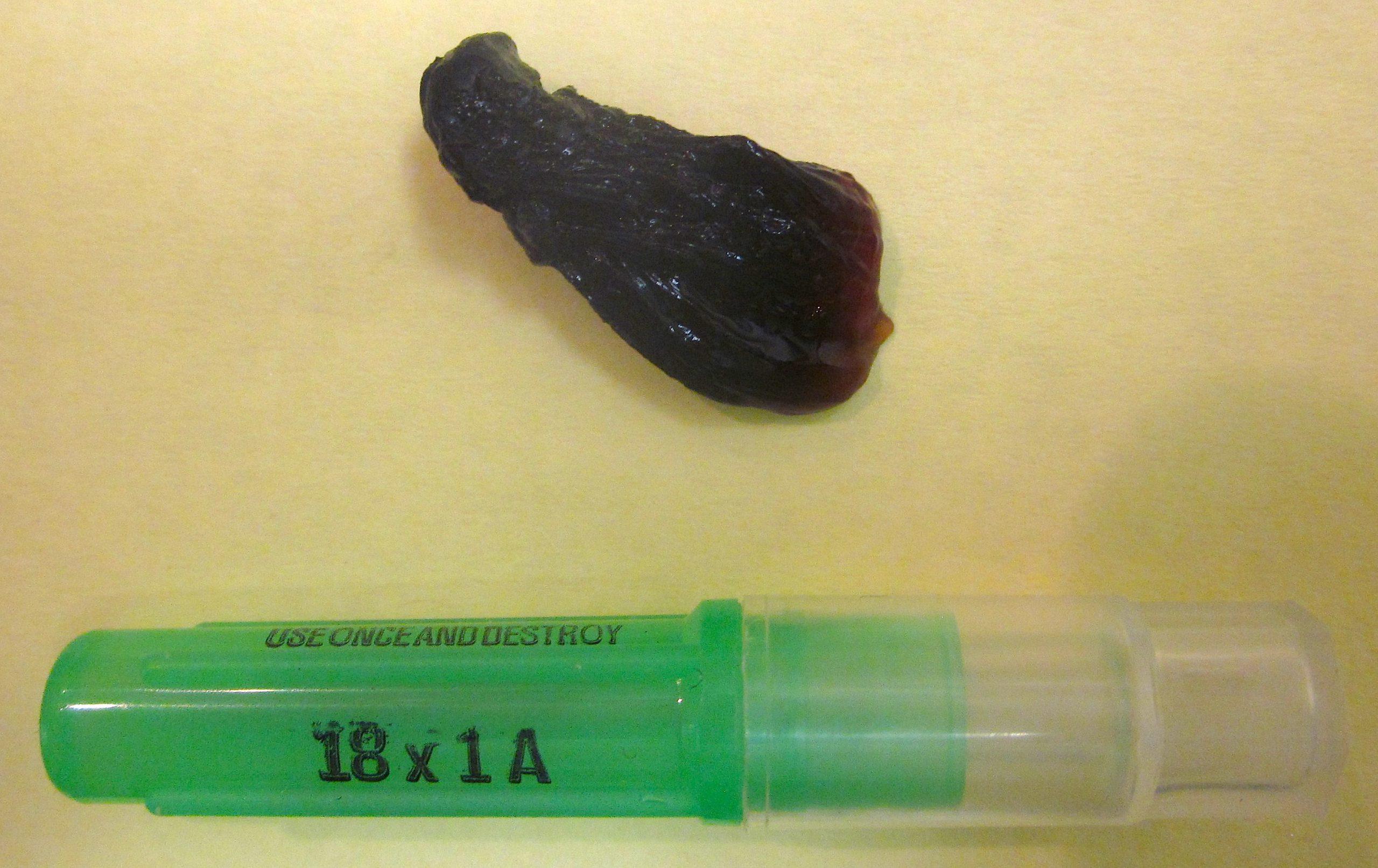
Perforated and inflamed Gb mucocele with localized peritonitis and minor pancreatitis
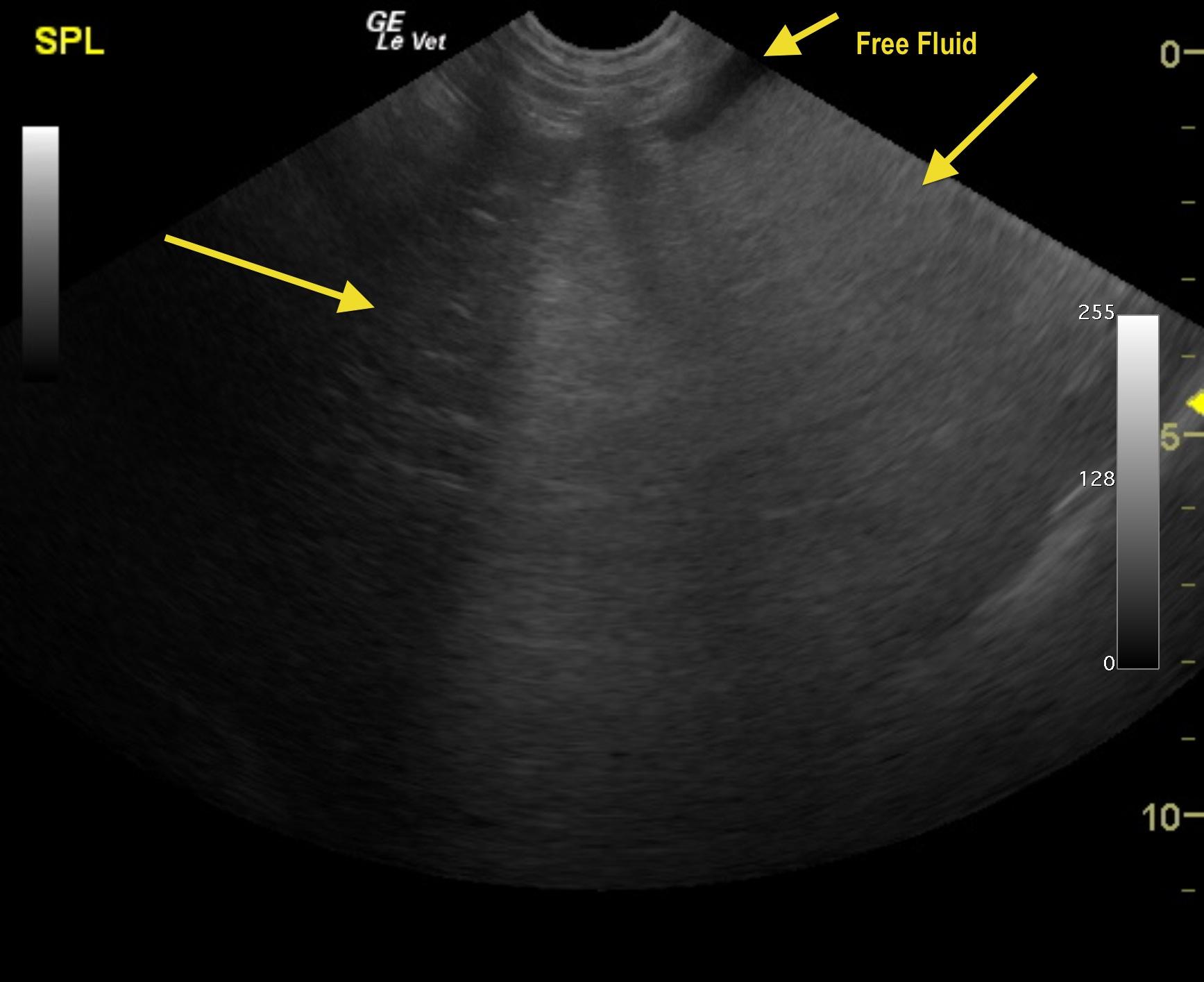
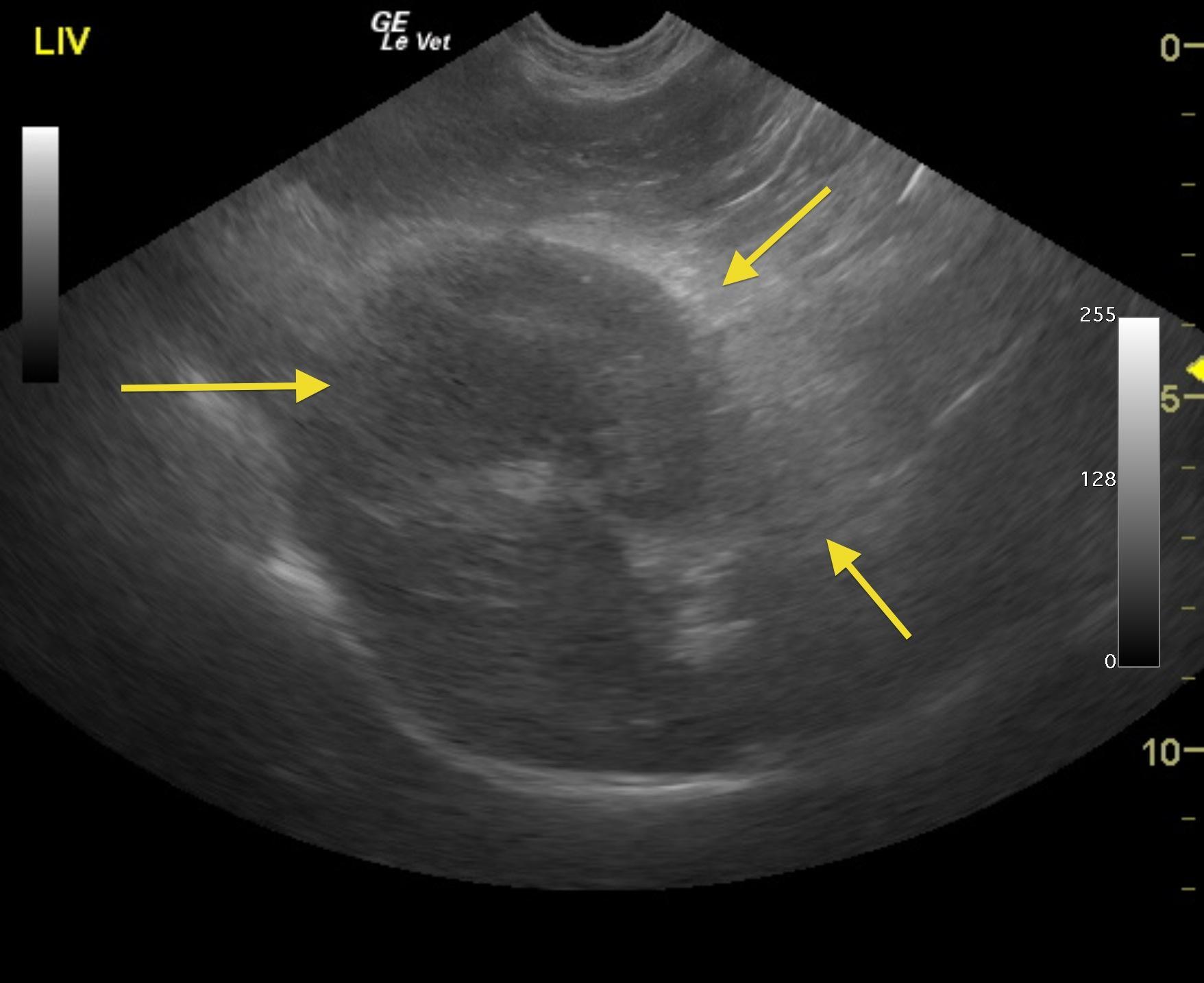
Inflamed or possibly ruptured gallbladder mucocele with adhesions in the region of the portal hilus. The common bile duct was not visible owing to adhesion pattern. Free fluid which is suggestive for possible perforation or inflammatory fluid deriving from the pancreas and gallbladder. This is a surgical emergency.
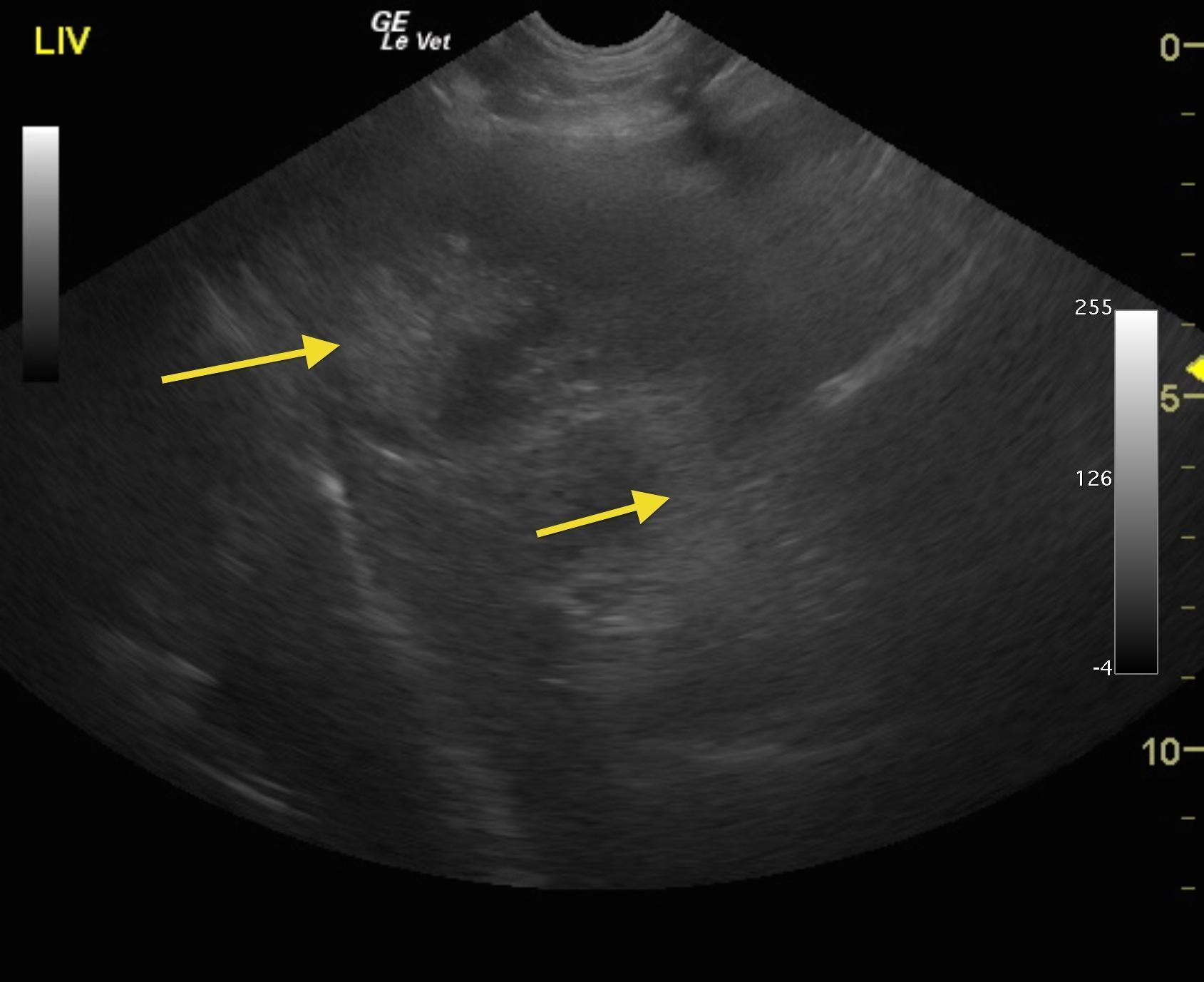
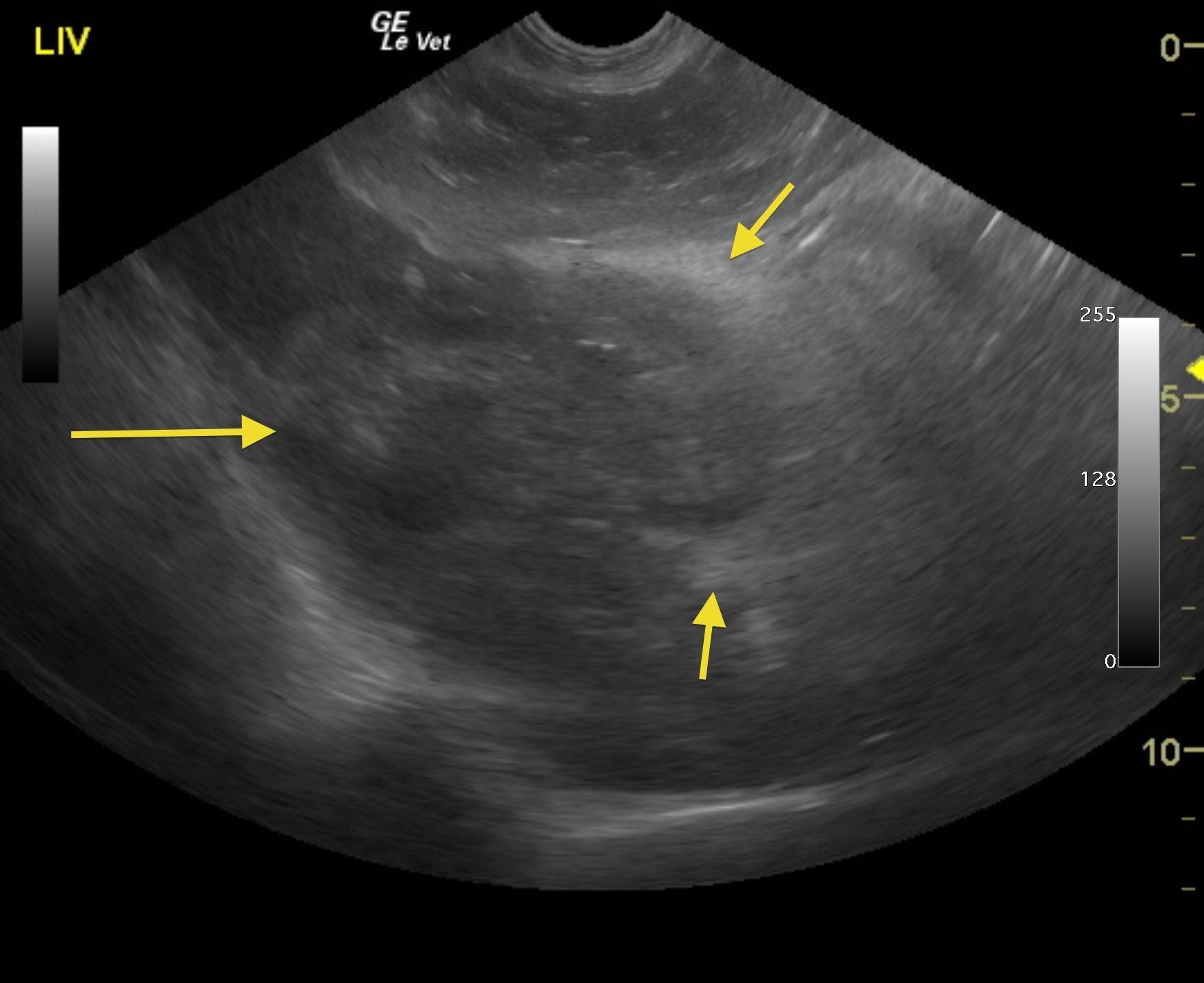
The liver in this patient was swollen and mildly irregular in contour. The gallbladder was dilated and egg shaped form with suspended, striating bile, completely inspissated. The wall and neck of the gallbladder was echogenic. Ill defined, inflamed fat was noted in the region. There were minor areas of free fluid was noted as well. Adhesions were noted throughout the region of the portal hilus and enveloped the pyloric outflow. The pancreas presented heterogenous changes in the right limb. The stomach presented some fluid accumulation and mild edema.