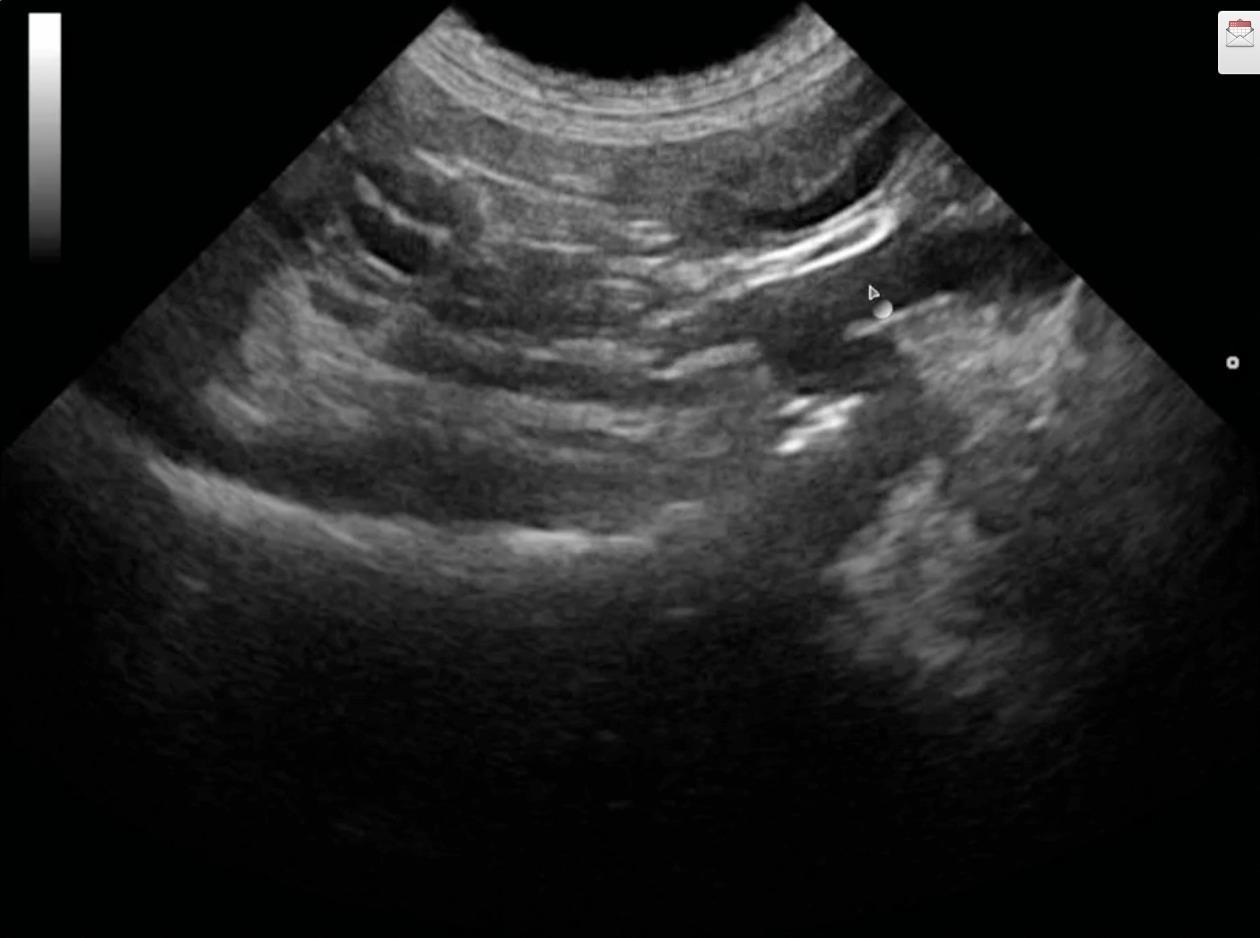
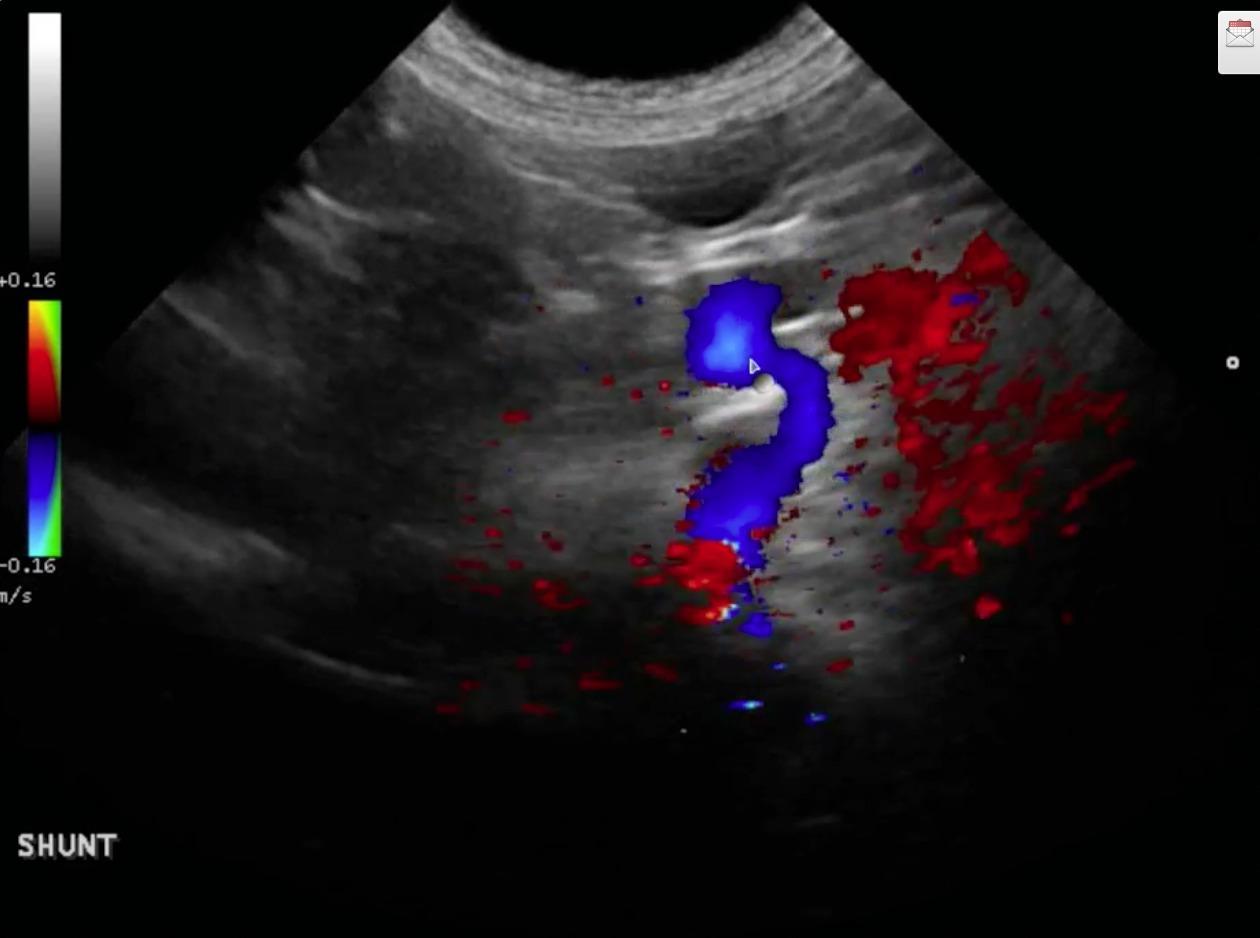
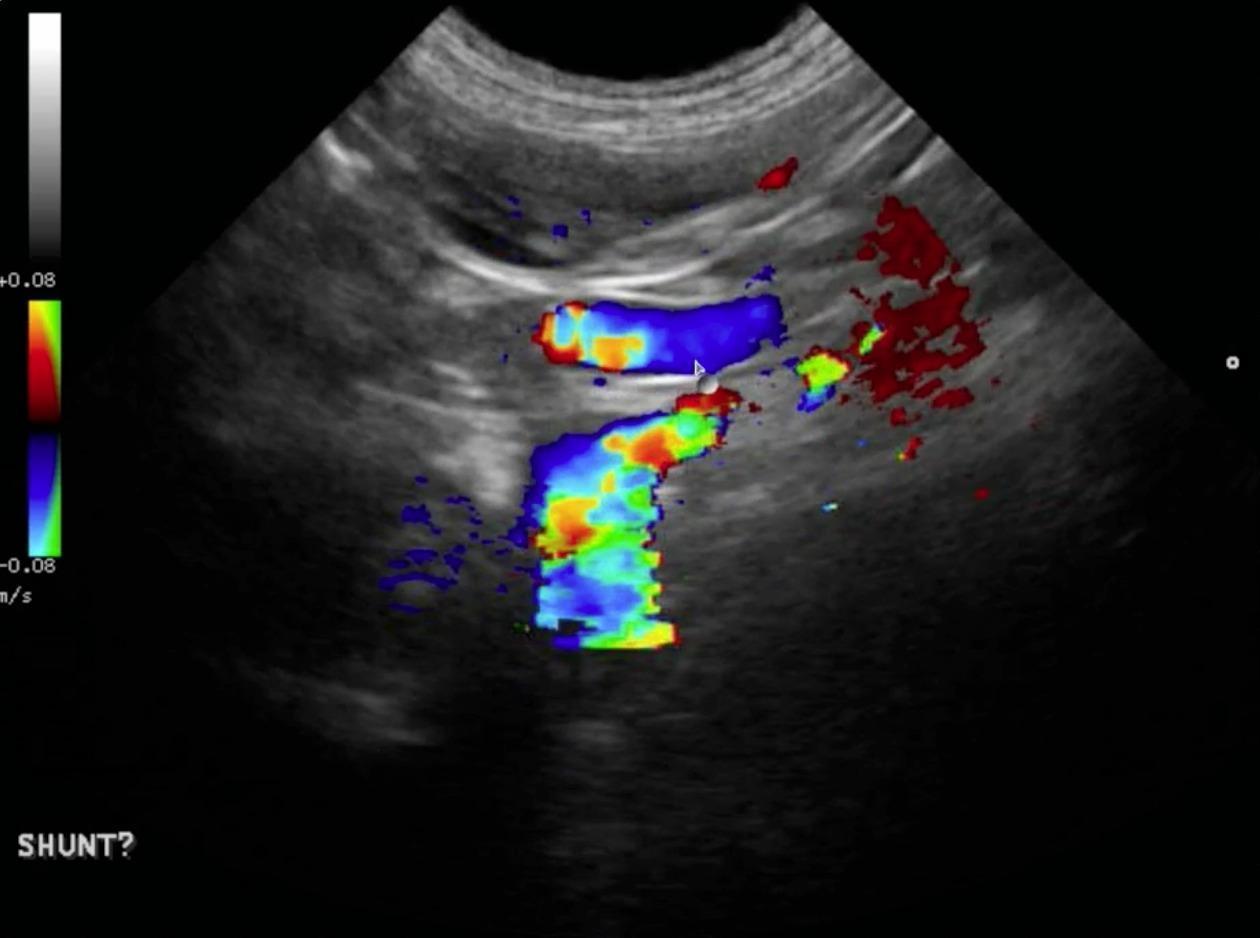
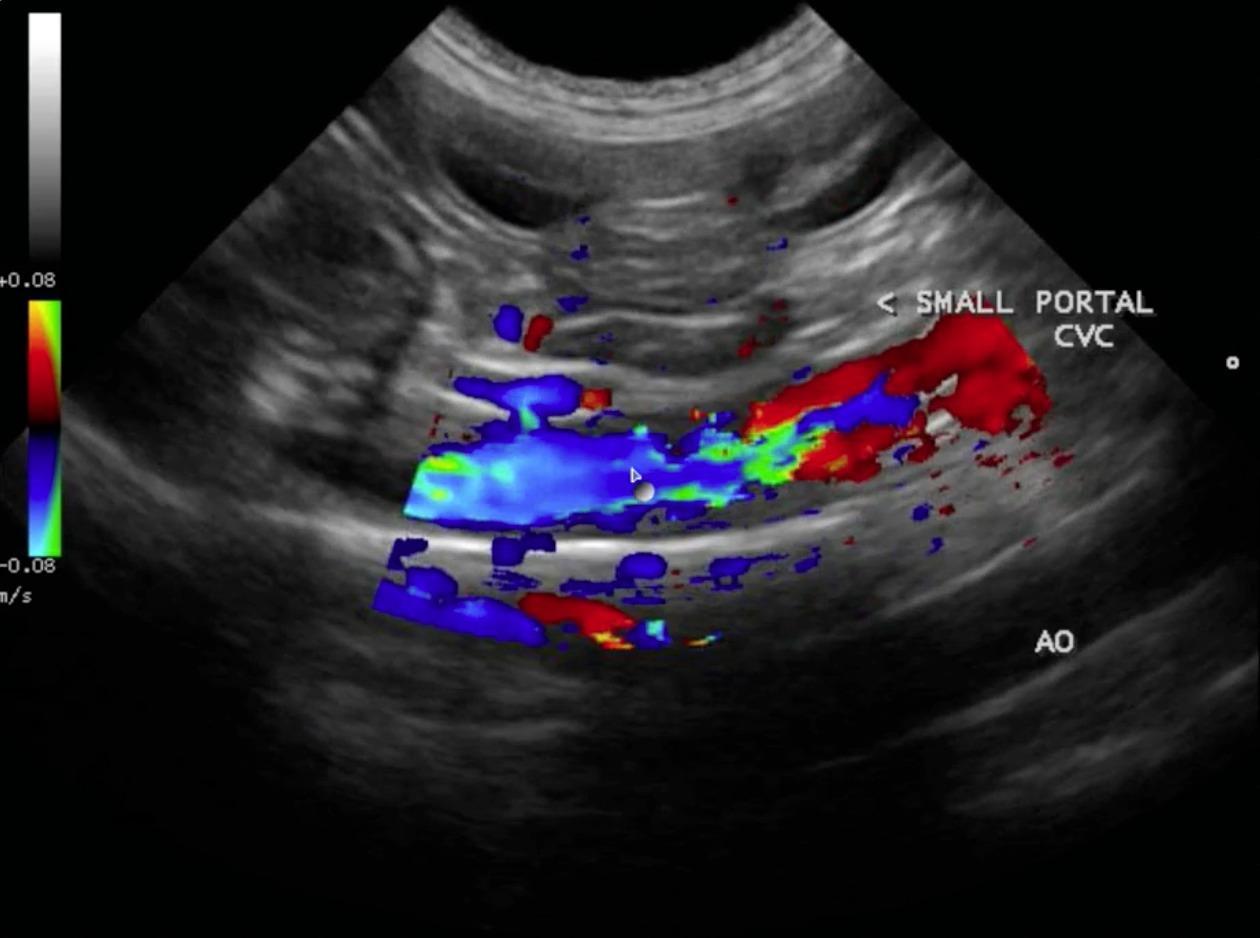
The patient was presented for vomiting 3-4 days prior. Was recently gagging, not urinating often despite normal drinking. The patient had a decreased appetite or was not eating at all and having innappropriate defecation in the house. Blood chemistry showed liver enzyme elevation and low BUN. Bile Acids test results were high at 464.6 umol/L. An abdominal ultrasound was recommended to rule out PSS, liver disease. possible infection- Lepto? (patient from Ontario, Canada), toxin, glomerulopathy, protein starvation, chronic non-obstructive FB, Addison, glomerulopathy, other.
The patient was presented for vomiting 3-4 days prior. Was recently gagging, not urinating often despite normal drinking. The patient had a decreased appetite or was not eating at all and having innappropriate defecation in the house. Blood chemistry showed liver enzyme elevation and low BUN. Bile Acids test results were high at 464.6 umol/L. An abdominal ultrasound was recommended to rule out PSS, liver disease. possible infection- Lepto? (patient from Ontario, Canada), toxin, glomerulopathy, protein starvation, chronic non-obstructive FB, Addison, glomerulopathy, other.