Although the prognosis is poor for this canine, this above formula resulted in THE best patient care for this pup!
The patient was presented for vomiting, lethargy, and painful cranial abdomen. Blood chemistry revealed BUN 5, glob. 4.7, ALT >1000, Alk.Phos. 1342, GGT 25, and T. bili 2.8. A STAT ultrasound was ordered and performed by ASNW with interpretation done by SonoPath.
The patient was presented for vomiting, lethargy, and painful cranial abdomen. Blood chemistry revealed BUN 5, glob. 4.7, ALT >1000, Alk.Phos. 1342, GGT 25, and T. bili 2.8. A STAT ultrasound was ordered and performed by ASNW with interpretation done by SonoPath.
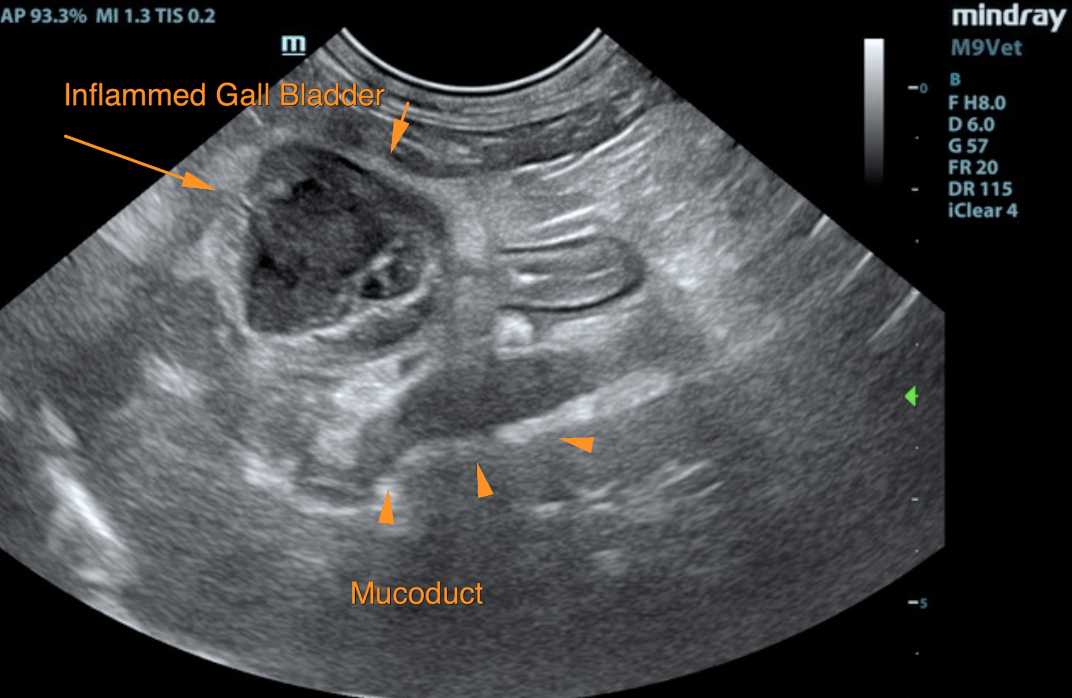
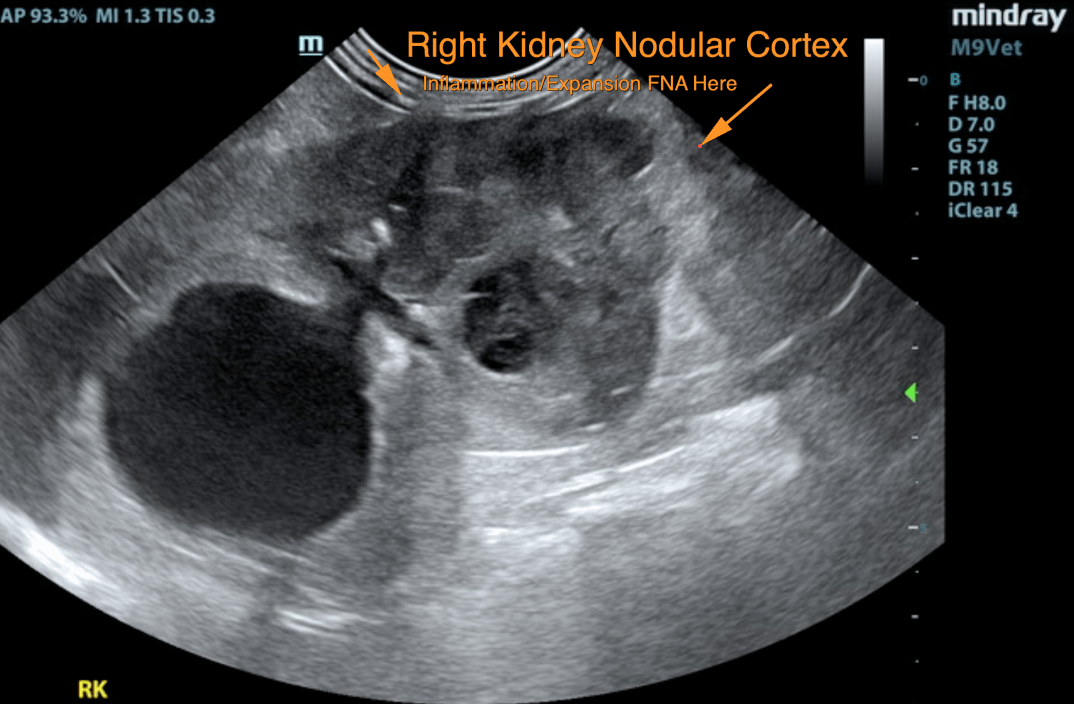
Renal carcinoma. Inflamed gallbladder mucocele and mucoduct.
The right kidney revealed multi-focal, hypoechoic nodular changes with regions of capsular expansion and enhanced peri-capsular fat. This meets neoplastic criteria. Concurrent polycystic changes were noted. The largest cyst at the cranial pole measured 3.56 x 3.54 cm. The patient may have passed a right renal calculus from the right kidney and it is now in the urinary bladder. Disruptive changes to the renal cortex may have occurred secondarily. Slight pyelectasia was noted as well. The left kidney revealed irregular cortical infarcts and pyelectasia. The left kidney measured 5.0 cm.
The gallbladder presented mucocele formation with regional inflammation. The common bile duct was dilated and measured 0.8 cm with mucous debris. This is consistent with mucoduct. Hyperechoic enhancement of the common bile duct was noted. Common bile duct wall thickening was noted.
Thoracic radiographs were taken following the ultrasound and a probable metastasis was visualized. The patient was then referred out to a specialty referral facility for stabilization, coagulation panel, and right kidney aspirate with cytology. Cytology confirmed renal carcinoma. Due to the poor prognosis, the patient will not be undergoing any surgical procedures and QOL/medical management has been elected. The patient is currently stable at home.