We all know what a classical Biliary mucocele looks like (picture from internet)  – but what if the images are not quite as clear.
– but what if the images are not quite as clear.
We all know what a classical Biliary mucocele looks like (picture from internet) – but what if the images are not quite as clear. How do you determine if there is an emerging biliary mucocele. What criteria do you use to consider an early mucocele.
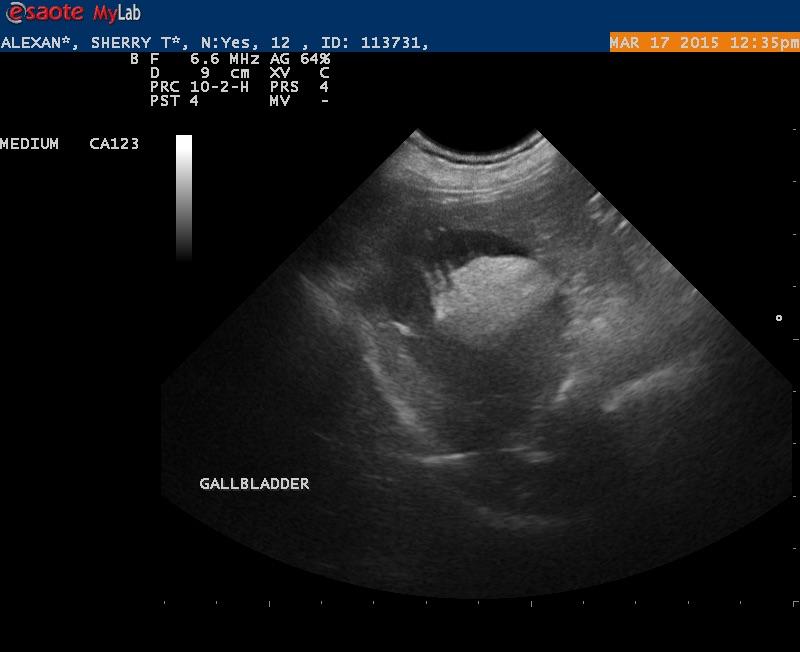
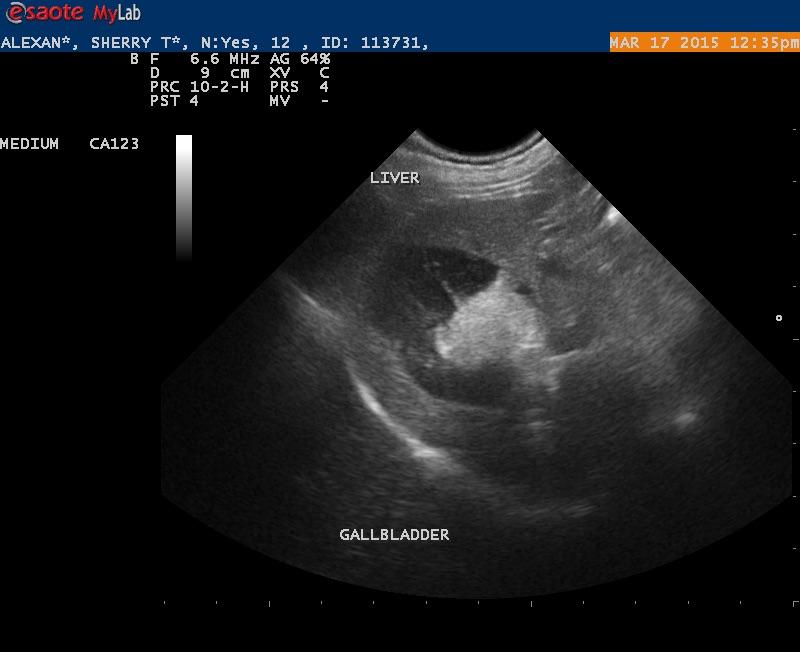
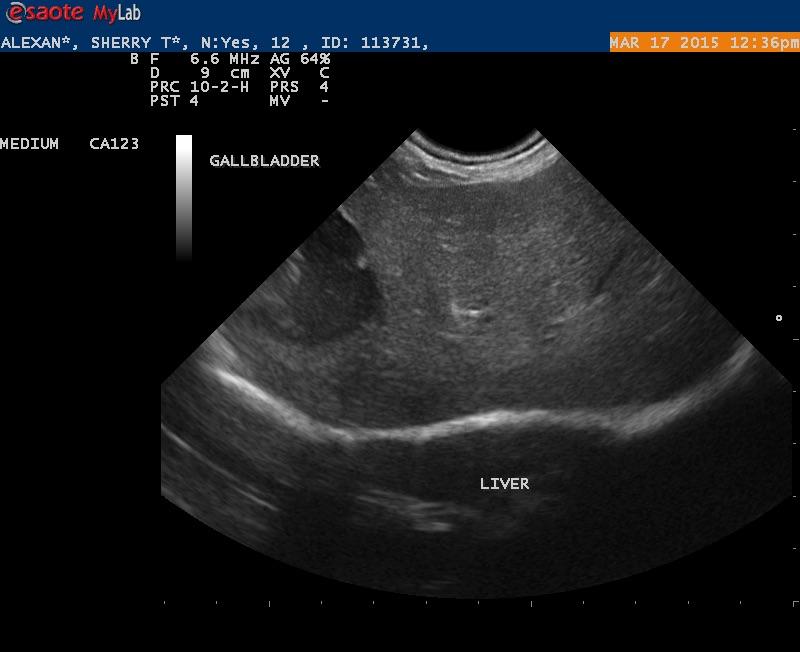
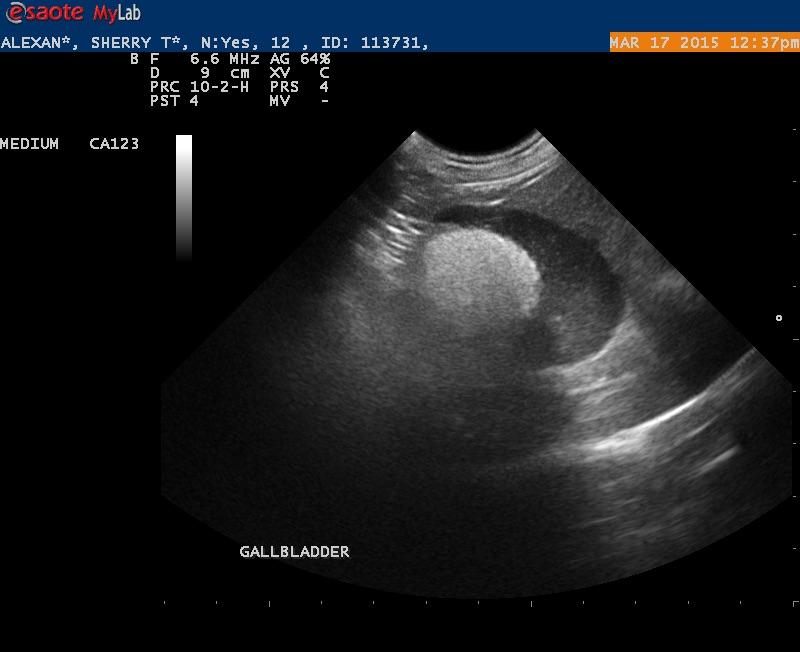
Alexandra is a 12 1/2 year old Minature Poodle that needs a dental prophy. She feels great. Routine lab work indicated an Alk Ptase of 730. That was the only abnormality. I did an abdominal scan and the only abnormality I saw was the gallbladder. Is this gallbladder filled with some insipated bile or should I be concerned about an emerging biliary mucocele?
12 responses to “Biliary Mucocele”
Bile is inpisated and
Bile is inpisated and starting to adhere so may well develop into a classic mucocele. Monitor the gall bladder for developement of a mucele, especially with the elevated ALP activity.
Bile is inpisated and
Bile is inpisated and starting to adhere so may well develop into a classic mucocele. Monitor the gall bladder for developement of a mucele, especially with the elevated ALP activity.
Thanks EL
Thanks EL
Thanks EL
Thanks EL
That was Remo..:) This is an
That was Remo..:) This is an atypical mucocele in my book. If you search mucocele in the basic search
http://sonopath.com/members/case-studies/search?text=mucocele&species=All
you will see tons of them that are classic and non classic many of which went into our study in 2009 on clinical parameters of surgical biliary disease. Could do a Gb motility study
http://sonopath.com/resources/instructional-library-sonopodcasts-interventional-procedures
to confirm its dysfuntional status… if anorexic , slowing down, ADR… and nothing else to explain the clinical signs then this Gb needs out in my opinion.
Our study on surgical biliary disease had a couple of cases that had no LE elevations whatsoever but removing the Gb resolved their signs. I agree with Remo in that SAP driving up is classic and the norm but on occasion that isnt the case. Remember the Gb has minimal cells to spill into the bloodstream so the liver parenchyma needs to be suffering to drive the LEs. If the Gb pathology is walled off then the LEs may not be a big deal. Our study showed this as well and the LEs are all over the map in these cases.
This Gb is overdistended, +/- 80% non mobile debris, striating bile… emerging mucocele if not a full blown one. Just not inflamed like the one from the internet in your title post…. not yet anyway:)
Take a look at the abstract… some day we will add the other 200+ ccases and get this published I hope.
ECVIM 2009 and “Defining a Gb mucocele”-survey both apply here:
http://sonopath.com/resources/research-publications
Nice post Randy! Sorry for t edelay I just got off the snowboard here in Keystone before the sonopath meeting starting tomorrow:)
That was Remo..:) This is an
That was Remo..:) This is an atypical mucocele in my book. If you search mucocele in the basic search
http://sonopath.com/members/case-studies/search?text=mucocele&species=All
you will see tons of them that are classic and non classic many of which went into our study in 2009 on clinical parameters of surgical biliary disease. Could do a Gb motility study
http://sonopath.com/resources/instructional-library-sonopodcasts-interventional-procedures
to confirm its dysfuntional status… if anorexic , slowing down, ADR… and nothing else to explain the clinical signs then this Gb needs out in my opinion.
Our study on surgical biliary disease had a couple of cases that had no LE elevations whatsoever but removing the Gb resolved their signs. I agree with Remo in that SAP driving up is classic and the norm but on occasion that isnt the case. Remember the Gb has minimal cells to spill into the bloodstream so the liver parenchyma needs to be suffering to drive the LEs. If the Gb pathology is walled off then the LEs may not be a big deal. Our study showed this as well and the LEs are all over the map in these cases.
This Gb is overdistended, +/- 80% non mobile debris, striating bile… emerging mucocele if not a full blown one. Just not inflamed like the one from the internet in your title post…. not yet anyway:)
Take a look at the abstract… some day we will add the other 200+ ccases and get this published I hope.
ECVIM 2009 and “Defining a Gb mucocele”-survey both apply here:
http://sonopath.com/resources/research-publications
Nice post Randy! Sorry for t edelay I just got off the snowboard here in Keystone before the sonopath meeting starting tomorrow:)
Thank you Remo and EL
I will
Thank you Remo and EL
I will look at the literature
Thank you Remo and EL
I will
Thank you Remo and EL
I will look at the literature
What is the normal range for
What is the normal range for GB fractional shortening at 15 minutes and 30 minutes. The synopsis did not specify.
What is the normal range for
What is the normal range for GB fractional shortening at 15 minutes and 30 minutes. The synopsis did not specify.
Unfortunately we dont have
Unfortunately we dont have established norms yet but if no movement is present then dysfunction is suspected. We have to have more numbers to create a normal and abnormal data set.
Unfortunately we dont have
Unfortunately we dont have established norms yet but if no movement is present then dysfunction is suspected. We have to have more numbers to create a normal and abnormal data set.