An 11-year-old SF Bichon dog was presented with a history of 3-4 days of lethargy, anorexia, and vomiting. Abnormalities on physical examination were tense abdomen, mild dehydration, and moderate dental tartar. Urinalysis (free-flow sample) showed inappropriate SG, (1.017), hematuria, and, pyuria. Abnormalities on CBC and serum biochemistry were leukocytosis, monocytosis, neutrophilia, azotemia, and hyponatremia.
An 11-year-old SF Bichon dog was presented with a history of 3-4 days of lethargy, anorexia, and vomiting. Abnormalities on physical examination were tense abdomen, mild dehydration, and moderate dental tartar. Urinalysis (free-flow sample) showed inappropriate SG, (1.017), hematuria, and, pyuria. Abnormalities on CBC and serum biochemistry were leukocytosis, monocytosis, neutrophilia, azotemia, and hyponatremia.
06_00104 Snowflake M Right ureteral obstruction with ureterolith
History
Clinical Differential Diagnosis
Renal – neoplasia, renoliths, pyelonephritis, nephritis Ureter – ureterolith Bladder – rupture with secondary uro-peritonitis Addison’s disease
Sampling
None
Sonographic Differential Diagnosis
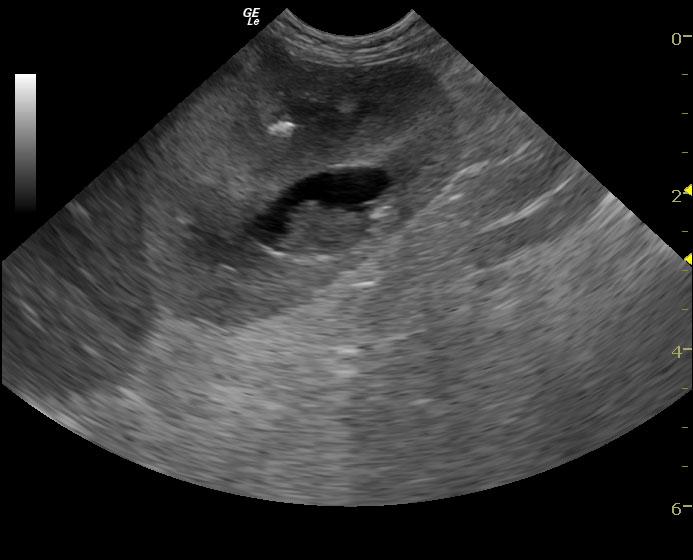
Bladder calculi. Right ureteral obstruction with secondary moderate pyelectasia and pyelonephrosis, likely infected renal pelvis. Renal calculi. Interventional radiology with stent placement in the right ureter would be an option in this patient with culture of the right renal pelvis. The other option would involve 24 hour IV fluid protocol, blood pressure, broad spectrum antibiotics and cystotomy and right nephrotomy with expectations of potential purulent right renal pelvis at the time of surgery in order to retrieve the right renal calculus that appears to be at the proximal portion of the right ureter just after the renal pelvis. It measured approximately 0.4 cm. It is not likely that this calculus will pass on its own.
Image Interpretation
The urinary bladder in this patient presented three to four 0.6-0.8 cm shadowing calculi with minor bladder wall thickening and suspended debris. Cystotomy would be warranted. This is most consistent with oxalate. The left kidney measured 3.0 cm with medullary calculi, dilation of the renal pelvis, and loss of corticomedullary detail. Chronic nephritis is likely. The right kidney revealed moderate hydronephrosis that measured 4.0 cm with a 2 x 1.5 cm pyelectasia of the right kidney with medullary calculus. The ureter was not overtly visible. Calculus was present within the proximal ureter in the right kidney causing obstruction. The renal pelvis presented echogenic debris, which is strongly suggestive of infection. A perinephric inflammatory pattern was noted; however, the right kidney appears to be significantly viable; therefore, intervention in order to save the right kidney would be recommended. Ultrasound-guided pyelocentesis with culture would be ideal. This could also be performed during surgery at the time of cystotomy.
Outcome
The owners decided not to pursue surgery or sampling at this time. No further outcome at this time.
Video
Patient Information
Blood Chemistry
- Azotemia
- Sodium, Low
CBC
- Monocytes, High
- Neutrophils, High
- WBC, High
Clinical Signs
- Anorexia
- Lethargy
- Vomiting
Exam Finding
- Dehydration
- Tense Abdomen
Urinalysi
- Blood Present
- Specific Gravity Low
- WBCs Present
Images