A 1-year-old intact male DSH with a history of VSD and pulmonic stenosis was presented for evaluation.
A 1-year-old intact male DSH with a history of VSD and pulmonic stenosis was presented for evaluation.
Ventricular Septal Defect and Reversal of Flow in a 1 year old Cat with Eisenmenger’s Physiology
History
Clinical Differential Diagnosis
Ongoing and stable VSD and pulmonic stenosis Reversal of VSD Right ventricular hypertrophy Myocardial failure
DX
Reversing VSD, mild pulmonic stenosis or compensatory elevated pa velocity.
Sonographic Differential Diagnosis
Reversing VSD, mild pulmonic stenosis.
Image Interpretation
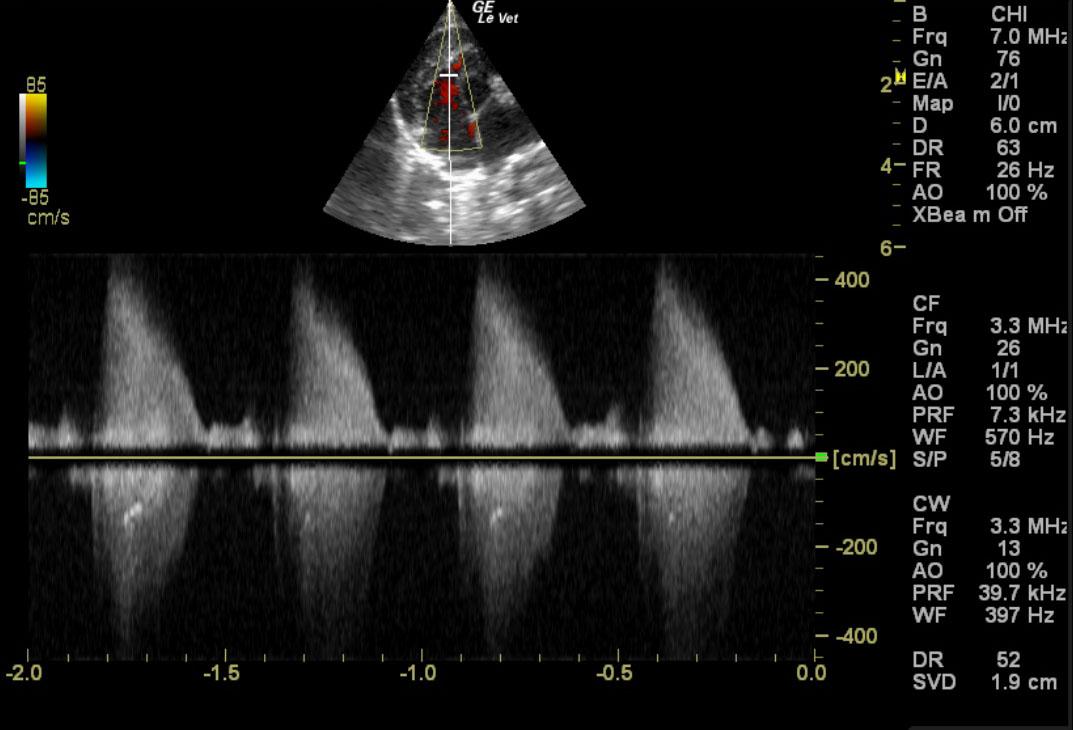
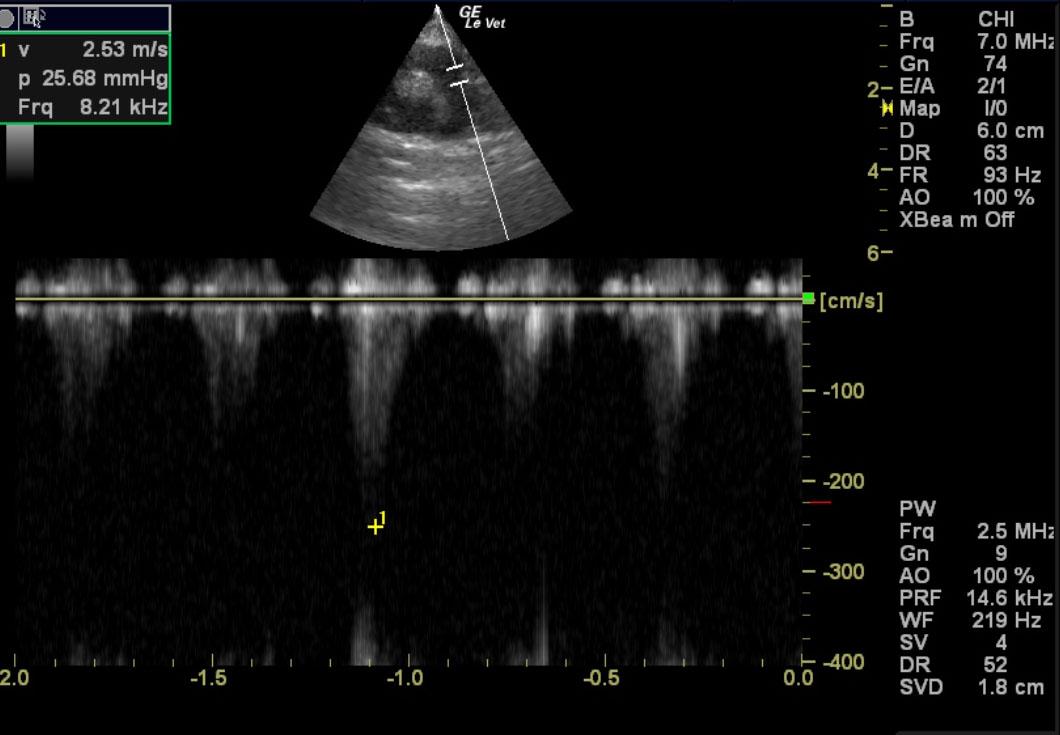
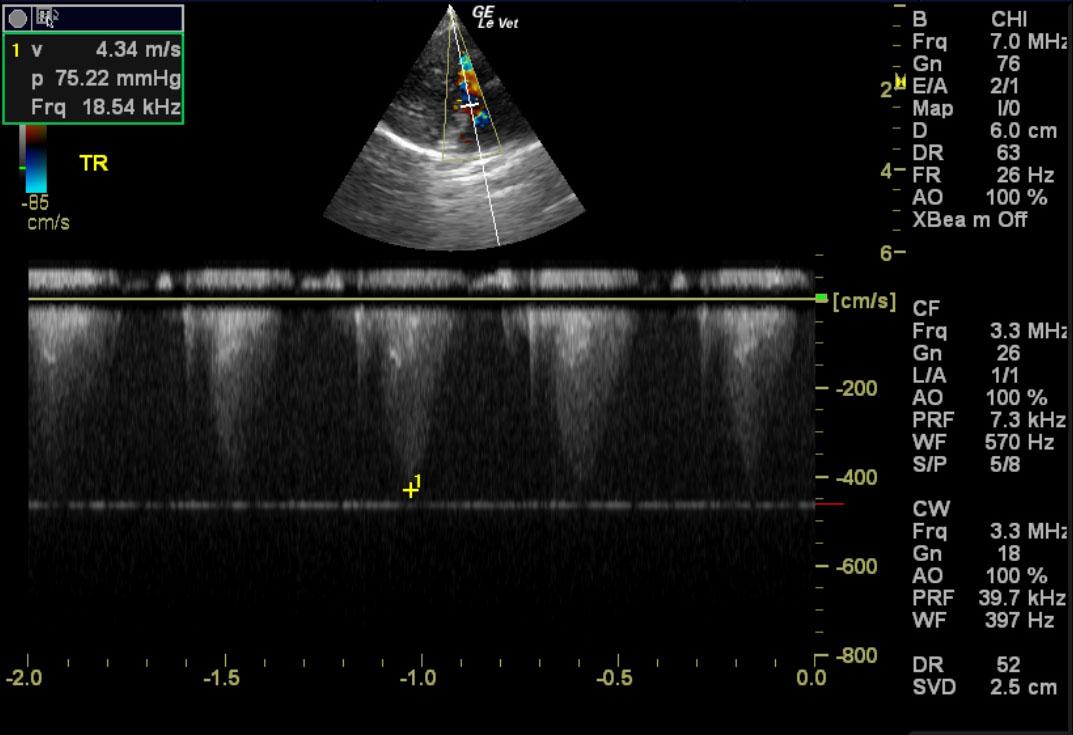
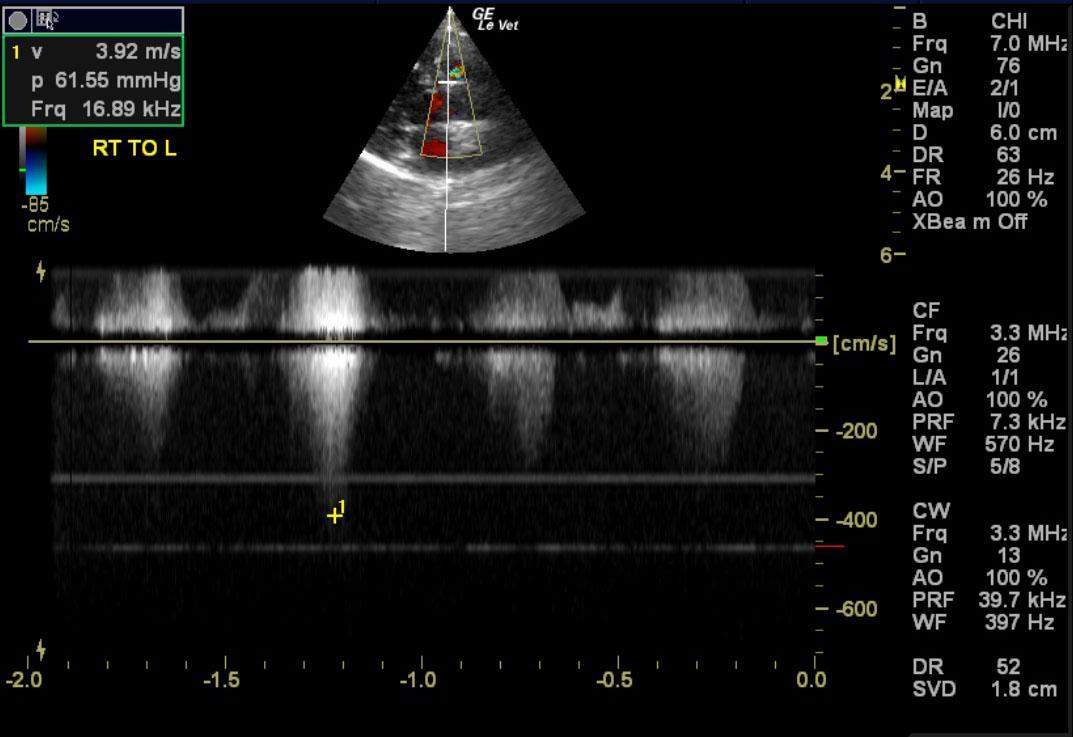
A ventricular septal defect was noted with both left to right and right to left shunting. This is consistent with reversing ventricular septal defect. The left to right shunting velocity was 3.72 m/sec. The right to left shunting velocity was 3.92 m/sec. The right atrium and right ventricle were dilated in this patient. Mildly increased right ventricular outflow velocity was noted. The pulmonic valve was mildly thickened. This is consistent with mild pulmonic stenosis or compensatory elevated velocity owing to the VSD. Tricuspid insufficiency was present. The tricuspid insufficiency was significant at 4.34 cm/sec. This is consistent with pulmonary hypertension. The left ventricle was thickened, yet the internal volume was normal. No free fluid or masses were noted. Tricuspid insufficiency 4.34 m/sec.
Outcome
If sedation is necessary in this case Torbutrol and Propofol combination would be recommended. Ace inhibitor therapy +/- Atenolol can be considered long term. The long term prognosis is very guarded.
Video
Patient Information
Patient Name : Bushmills M
Age : 1 Year
Gender : Male, Intact
Species : Feline
Liz Wuz Here : Yes
Status : Complete
Code : 15-00148
Images