A 13-year-old FS Greyhound with a history of renal insufficiency was presented for collapse, lethargy, and inappetance. The patient was febrile. Abnormalities on CBC and serum biochemistry were monocytosis, elevated liver enzymes, azotemia, and elevated CPK of 22730. T4 was low.
A 13-year-old FS Greyhound with a history of renal insufficiency was presented for collapse, lethargy, and inappetance. The patient was febrile. Abnormalities on CBC and serum biochemistry were monocytosis, elevated liver enzymes, azotemia, and elevated CPK of 22730. T4 was low.
Addison’s disease, sepsis, neoplasia, acute renal decompensation, myocarditis.
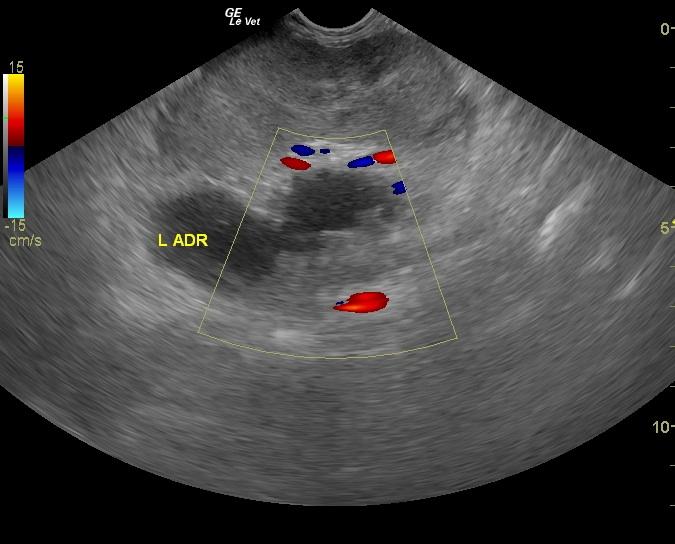
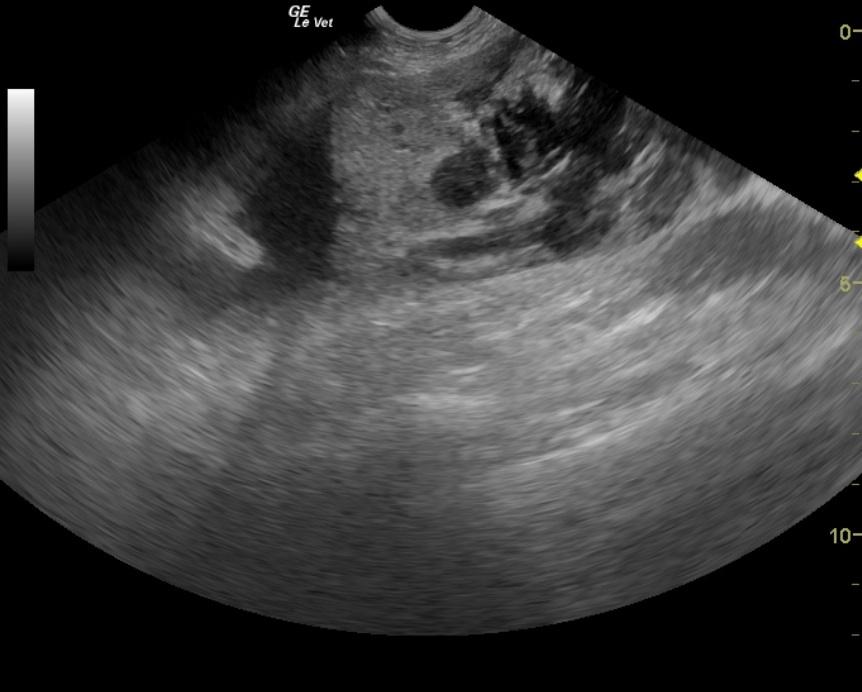
Left adrenal gland mass that had aggressively invaded the vena cava.
The abdomen in this patient presented a large left adrenal echogenic mass displacing the left kidney and invading the phrenic abdominal vein and into the vena cava. There was a lack of color flow signals within the mass suggestive of necrosis or hematoma within the mass itself (Still image 1). A dilated and infiltrated vena cava filled with tumor and likely attached thrombus was also evident (Still image 2 and videos 3 and 4). The mass occupied the vena cava and extended caudally to the iliac bifurcation and cranial to the diaphragm. Expansion of the vena cava was noted at 2.5 cm, which is 2 ВЅ times the width of the aorta. Minimal blood flow was present.