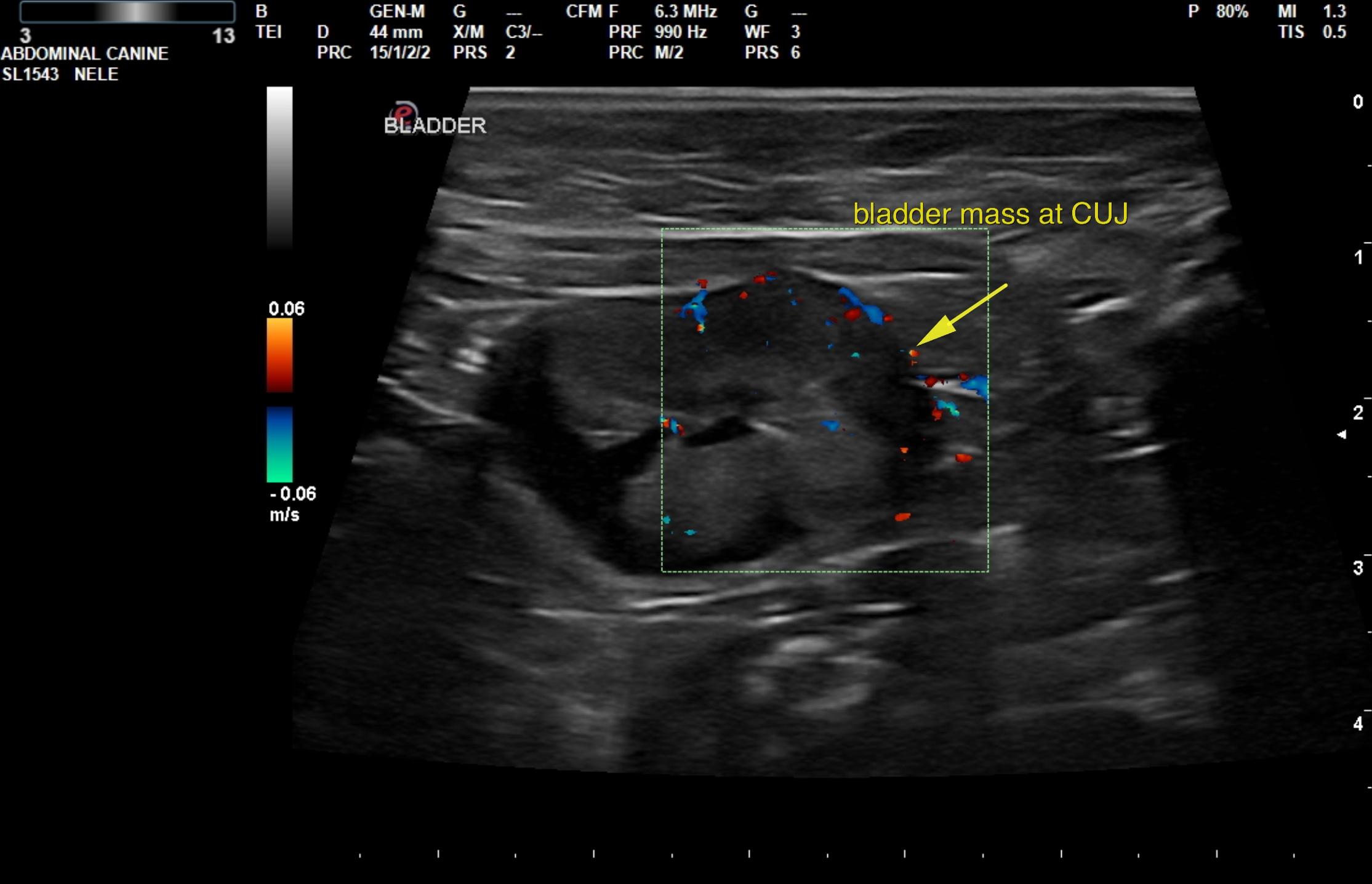
This 11 year old MN DS cat has a history of hematuria/stranguria/pollakuria of 10 months duration.
CBC/Chem: BUN 59, WBC low 2900
Urinalysis: USPG 1.016, protein +1, blood +3, WBCs 2-3/hpf, RBCs 21-50/hpf
This 11 year old MN DS cat has a history of hematuria/stranguria/pollakuria of 10 months duration.
CBC/Chem: BUN 59, WBC low 2900
Urinalysis: USPG 1.016, protein +1, blood +3, WBCs 2-3/hpf, RBCs 21-50/hpf