The patient is a 6 year old MN Corgi dog with acute overnight paralysis.
Physical exam – non-ambulatory paralysis; loss of deep pain in right hind; lower motor neuron signs; back pain
The patient is a 6 year old MN Corgi dog with acute overnight paralysis.
Physical exam – non-ambulatory paralysis; loss of deep pain in right hind; lower motor neuron signs; back pain
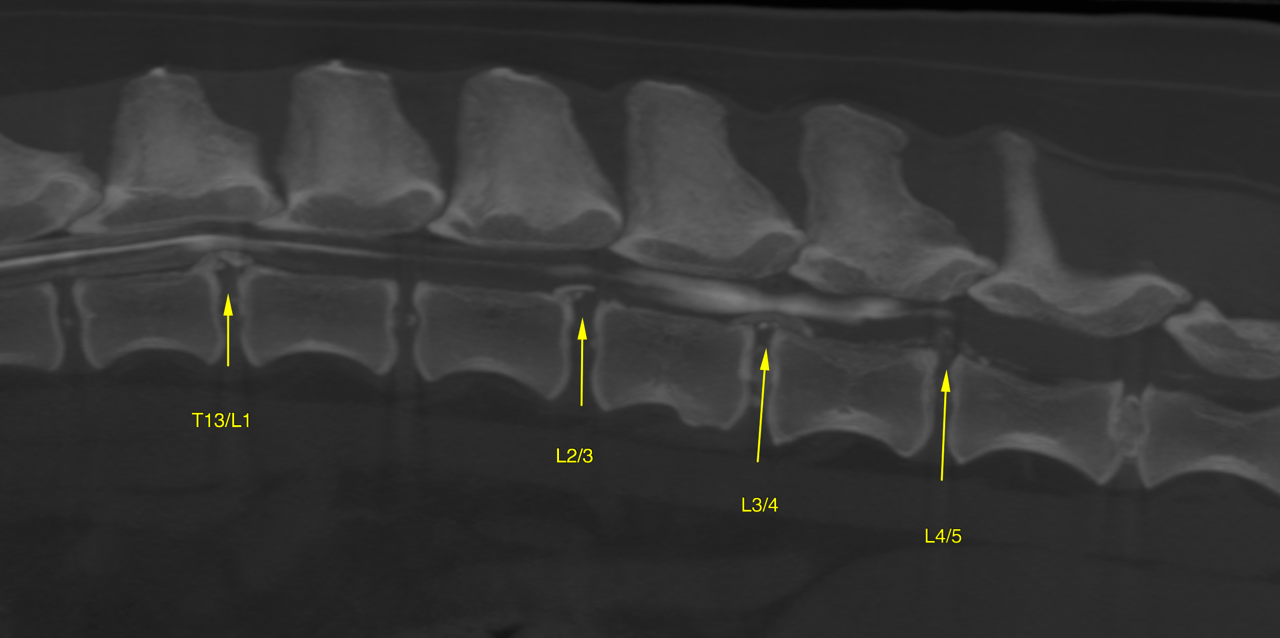
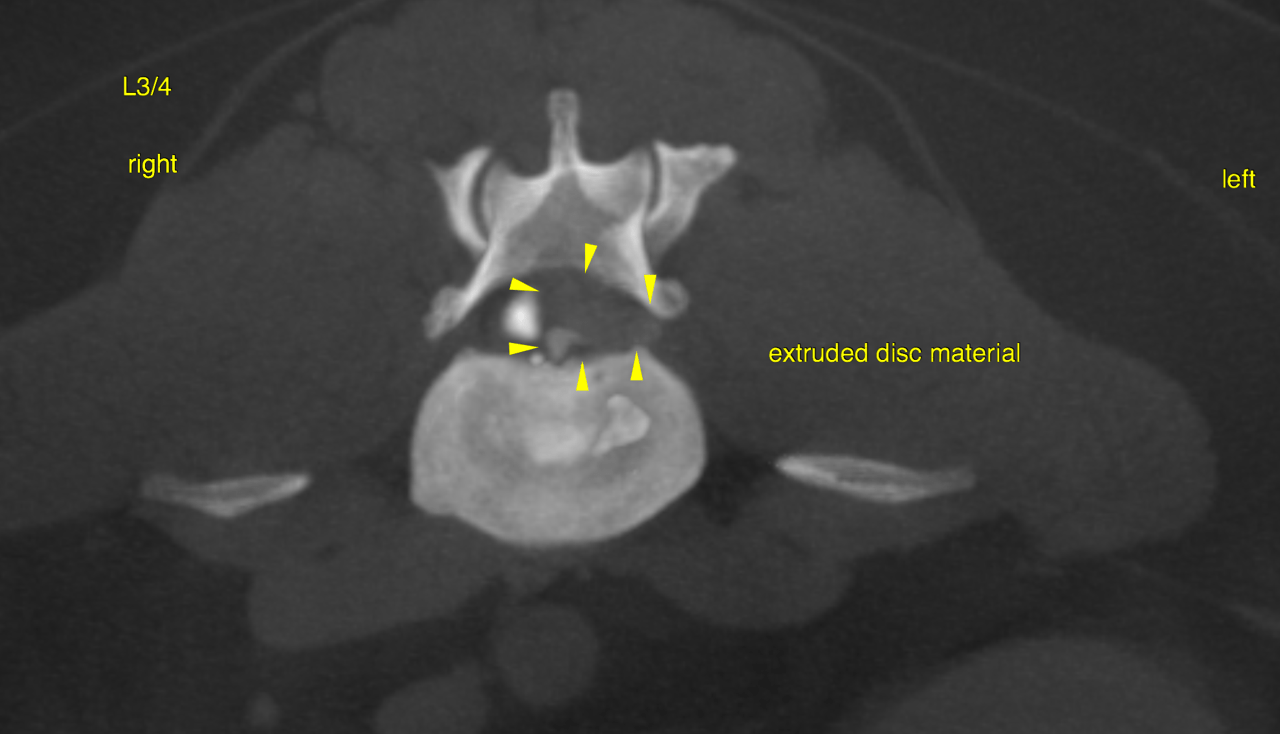
Acute severe lateralized disc extrusion with severe compressive myelopathy level with L3/4
CT of the spine – There is a vetriculogram and canalogram, which reveals irregular widening beyond the
normal central canal width of 1 mm throughout the cranial and mid cervical spine.
Level with L3/4 a severe acute extrusion of heterogeneously hyperattenuating disc
material is noted. The extruded disc material is located within the left epidural space,
the spinal cord is displaced to the right. The extrusion occupies 75 % of the central
canal diameter and extends cranially as well as caudally beyond the disc space by one
third of the length of the vertebral bodies of L3 & L4. There is evidence of severe
compressive myelopathy. The material extends into the entrance zone of the left
neuroforamen.
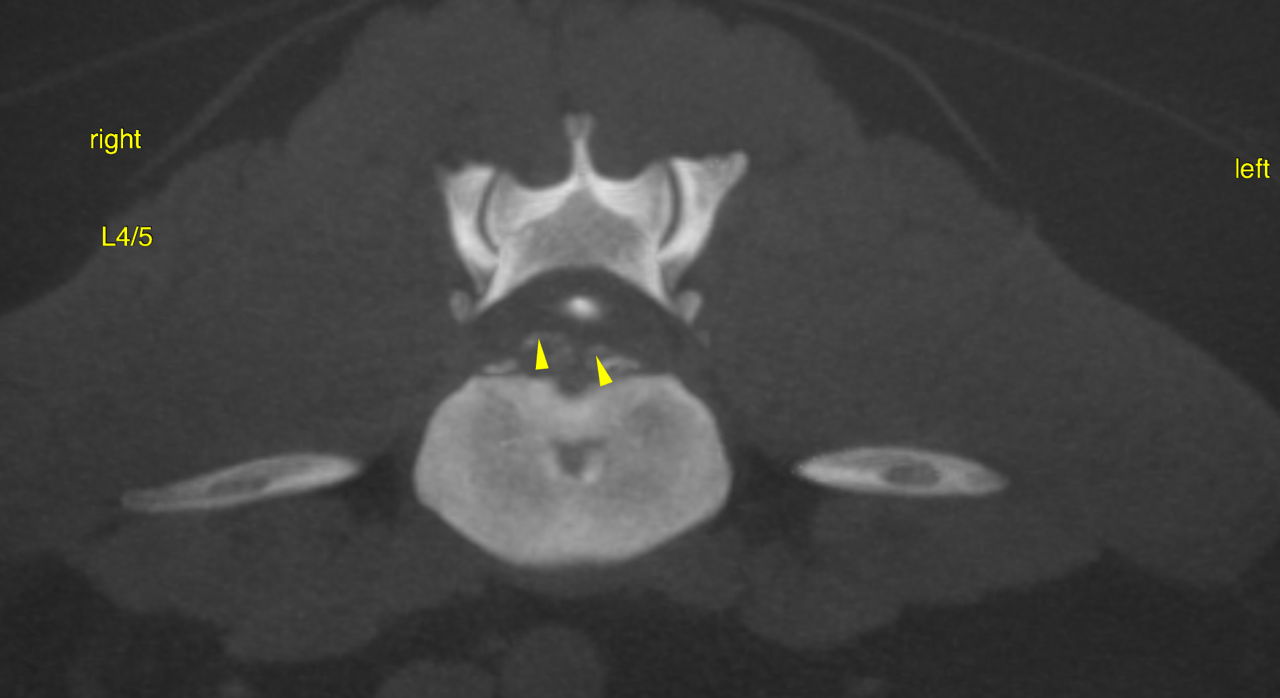
An older organized extrusion causing moderate compressive myelopathy is noted level
with L4/5. The extruded material is mainly centrally located within the ventral epidural
space with slight deviation to the right.
There is evidence of old organized disc extrusions within the ventral epidural space
level with T13/L1 leftsided with mild compressive myelopathy as well as at L2/3
centrally located with mild compressive myelopathy.
There is an emerging Spondylosis deformans at the T5/6 disc space.
Multifocal intervertebral disc degeneration as a function of generalized chondroid disc
degeneration as typical in chondrodystrophic dogs is noted throughout the spine. Bilateral moderate hip dysplasia with moderate coxofemoral osteoarthritis is noted.
The urinary bladder is severely distended.
Surgical decompression is warranted. A leftsided approach should be preferred.
Moreover a moderate compressive myelopathy is caused by a subacute to chronic
extrusion level with L5/6.
Surgical decompression may be considered because of the moderate degree of spinal
cord/Cauda equina compression at the same time.
The old organized extrusions at T13/L1 and L2/3 do not require surgical
decompression at this point.