This 8 year old MN Siamese cat has a history of persistent coughing, upper respiratory stridor and congestion of 7 months duration. During a November 2015 visit there was self induced alopecia noted. The CXR were unremarkable per radiologist. Abdominal radiographs showed bilateral small kidneys. Treated with prednisone for 10 days and clavamox. The coughing persisted through late November and was treated with Convenia and depomedrol.
This 8 year old MN Siamese cat has a history of persistent coughing, upper respiratory stridor and congestion of 7 months duration. During a November 2015 visit there was self induced alopecia noted. The CXR were unremarkable per radiologist. Abdominal radiographs showed bilateral small kidneys. Treated with prednisone for 10 days and clavamox. The coughing persisted through late November and was treated with Convenia and depomedrol.
The computed tomographic findings are compatible with mild bilateral unspecific non-destructive rhinitis and sinusitis causing significant upper airway obstruction. Mild reactive lymphadenitis is seen as well.
CT of the head and thorax –
Head:
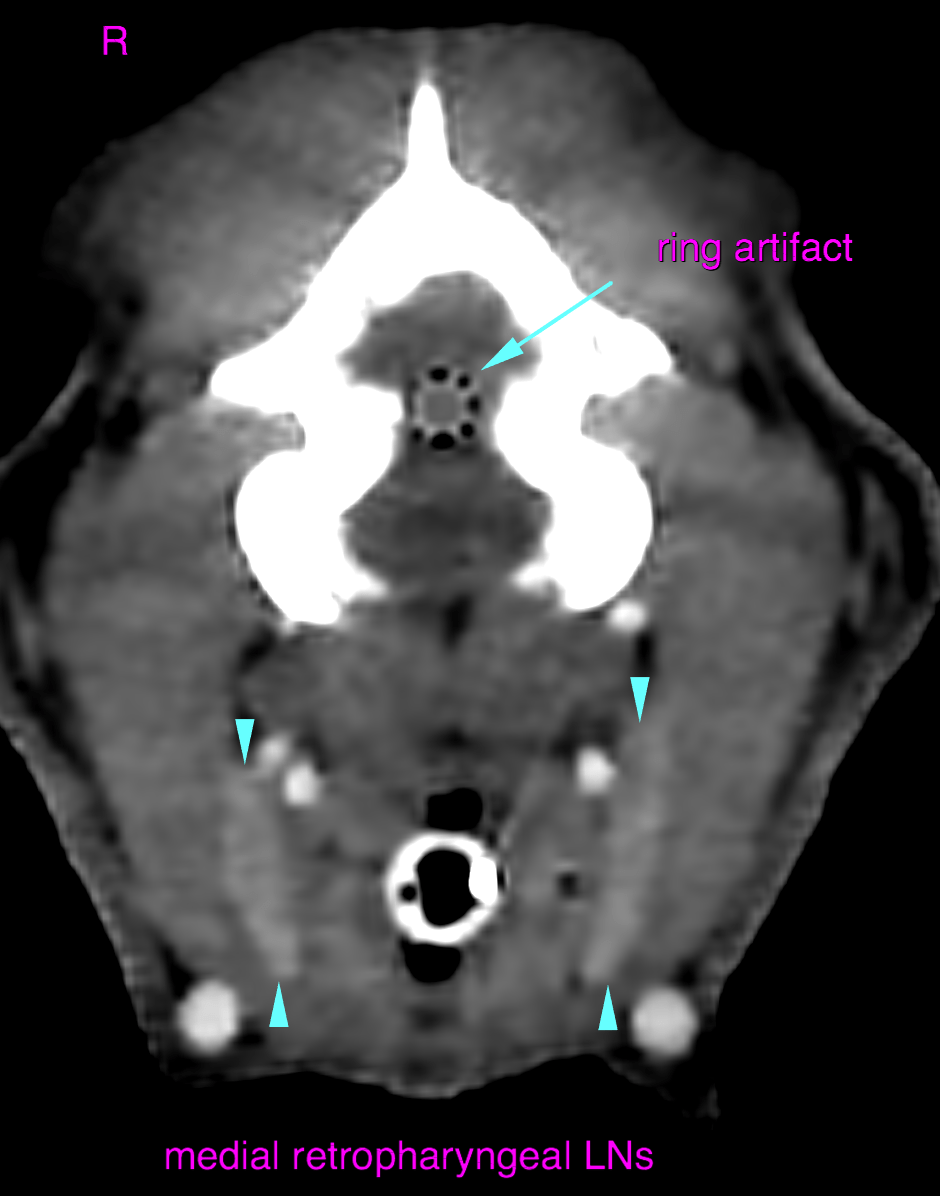
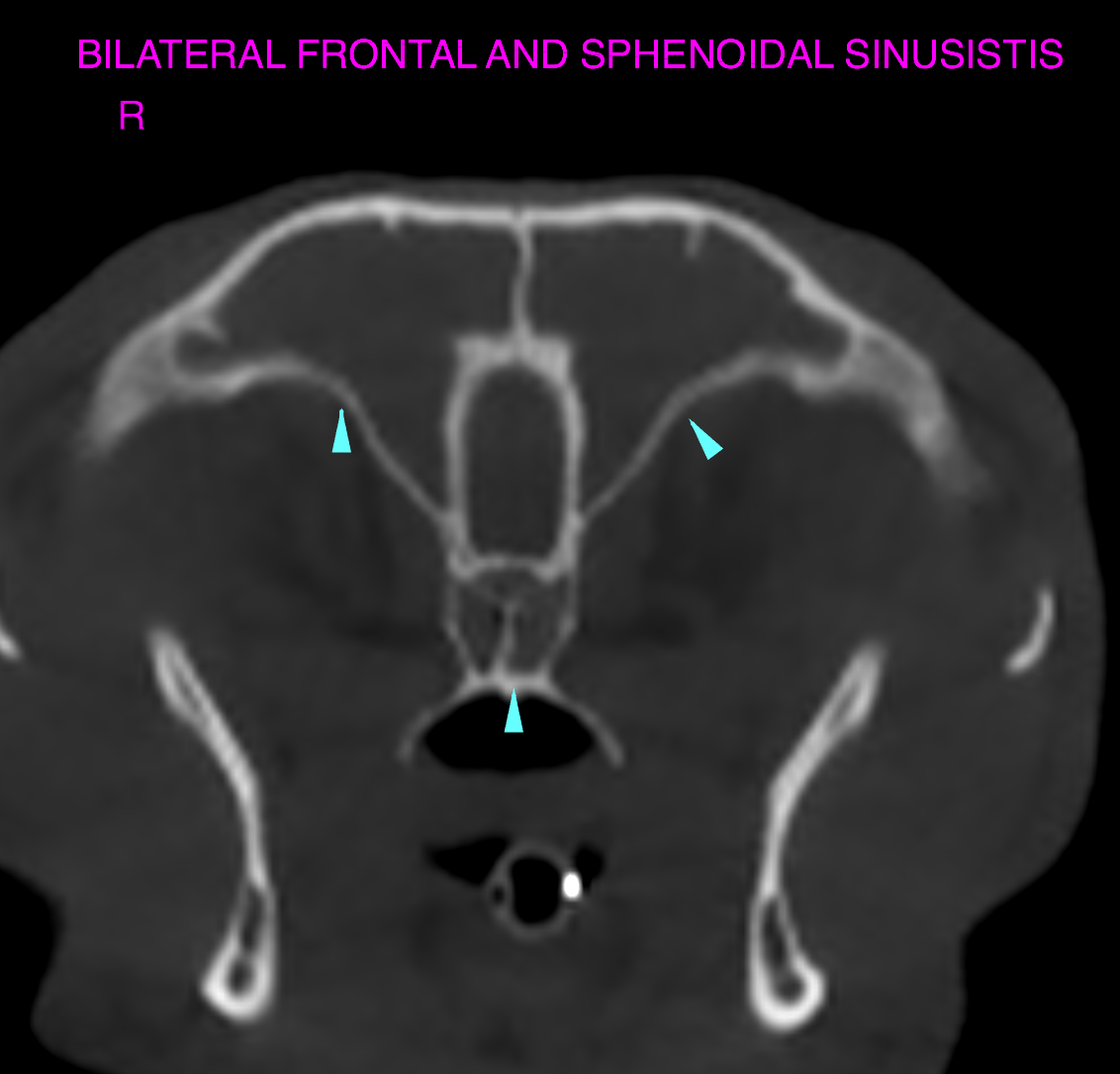
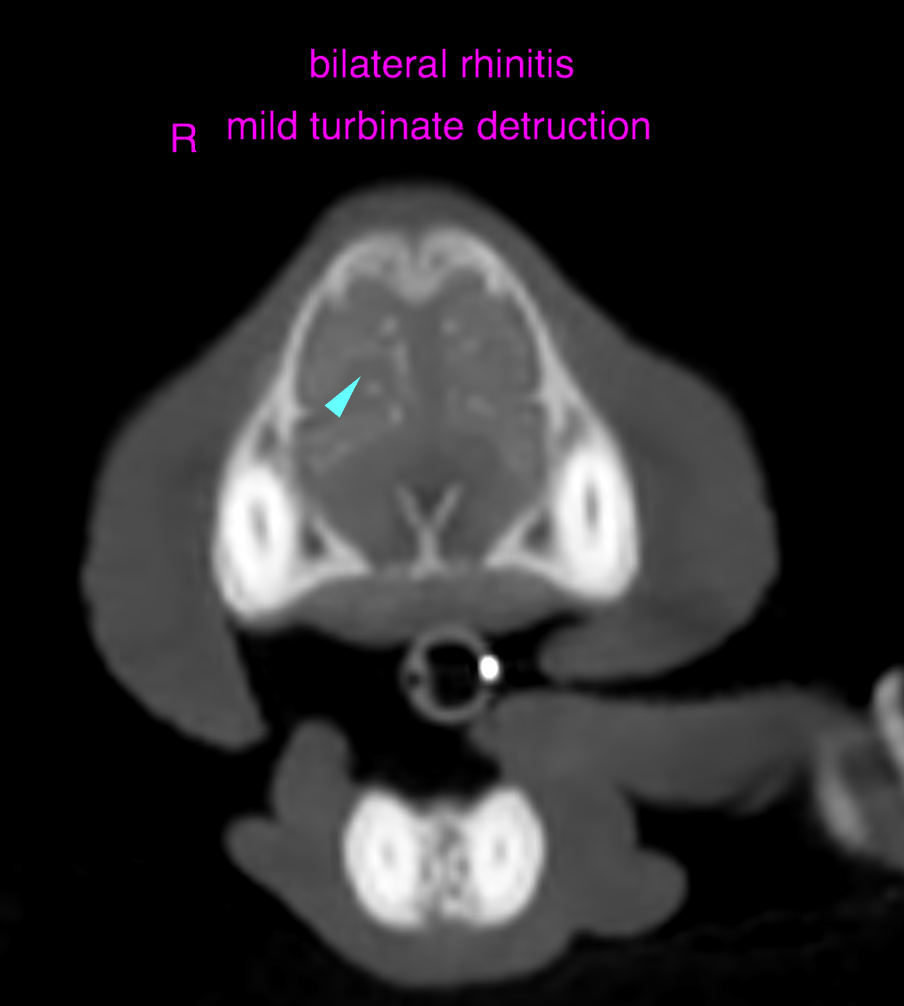
The computed tomography of the head reveals generalized and bilateral thickening of the mucosal lining of the nasal turbinates as well as a moderate amount of gravity-dependent non-enhancing nasal secretions occupying both nasal cavities. Only very mild focal turbinate destruction is seen. Fluid attenuating secretions occupy both frontal and sphenoidal sinuses. The right submandibular and medial retropharyngeal lymph nodes present mild symmetrical enlargement with maintained short-to-long axis ratio < 0.5 and regular contrast enhancement pattern.
Thorax:
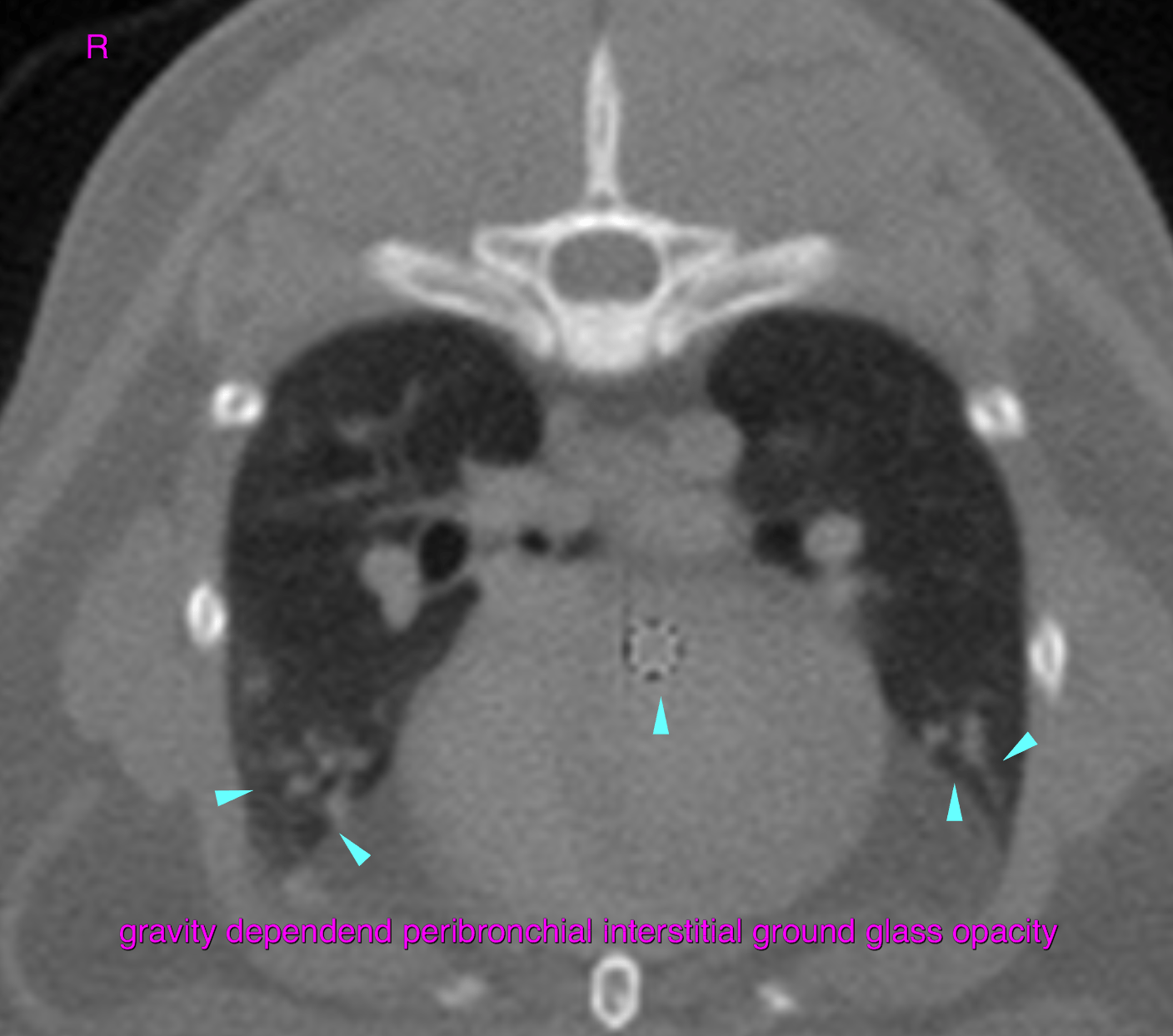
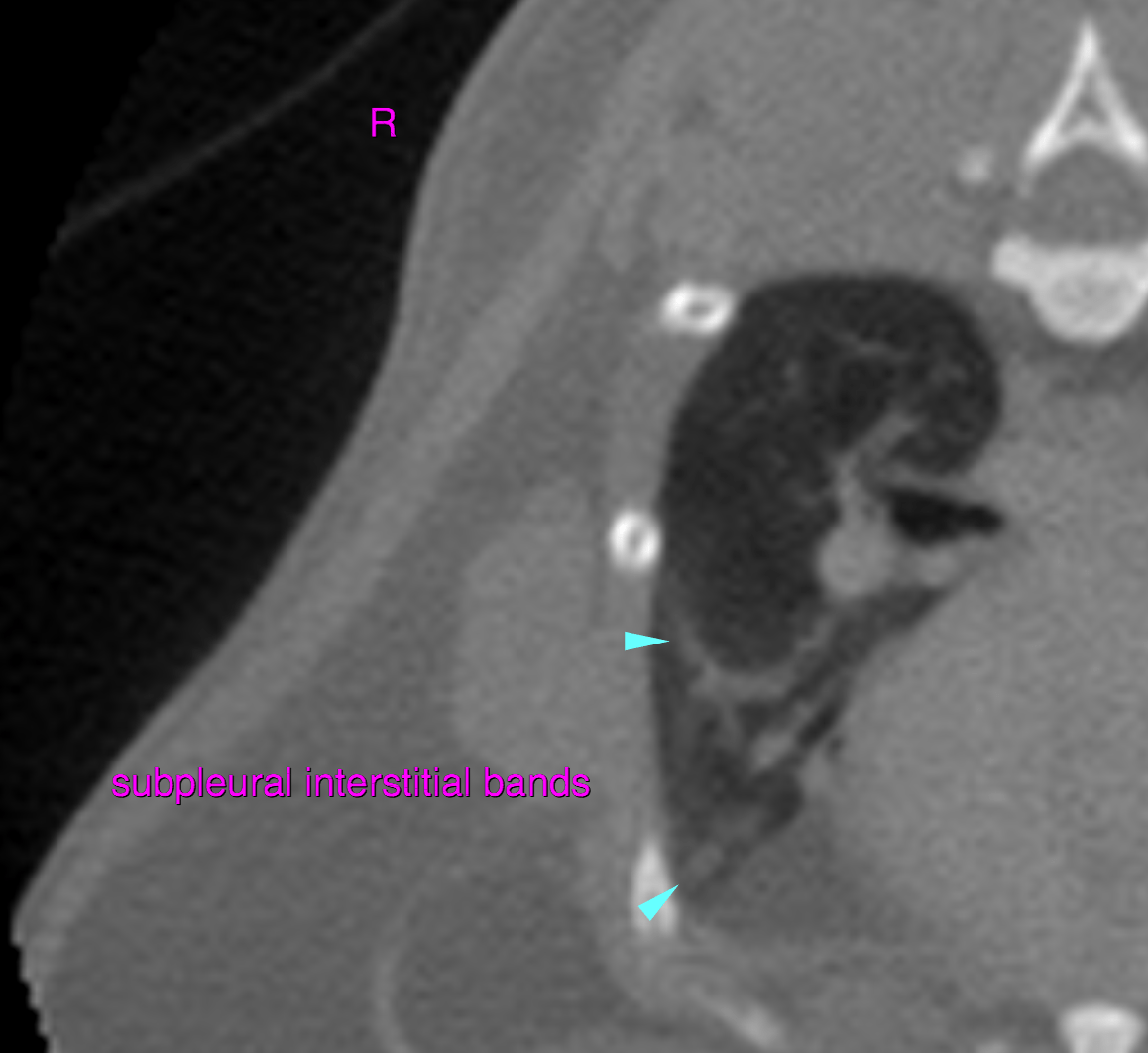
Within the ventral aspects of the lung multifocal gravity-dependent peribronchial interstitial ground glass opacities are noted as well as several interstitial bands with subpleural emergence.
Potential underlying causes include bacterial rhinitis and viral rhinitis with bacterial superinfection. Typical findings of fungal rhinitis are lacking here. Theoretically emerging fungal rhinitis/recent fungal superinfection cannot be ruled out entirely. Recent antimicrobial treatment may reduce the degree of mucosal thickening and amount of nasal/sinus secretions.
Part of the lung changes may relate to pulmonary atelectasis under general anesthesia. However, mild signs of chronic or healed bronchopneumonia with scarring of the pulmonary interstitium are noted.
Rhinoscopy with sampling to obtain bacterial and fungal cultures & histopathology is advised for further definition and to adjust the therapeutic management appropriately.
Consider to rule out relevant pulmonary superinfection by means of bronchoalveolar lavage at the same time.