This 12 year old FS Border Collie mixed dog presented with intermittant lameness of the left front leg of approximately one year duration
Physical Exam: Pain in the left shoulder and left elbow
This 12 year old FS Border Collie mixed dog presented with intermittant lameness of the left front leg of approximately one year duration
Physical Exam: Pain in the left shoulder and left elbow
Emerging calcifying insertional tendinopathy of the right supraspinatus muscle. Mild effusion and synovitis of the right stifle joint.
Ultrasound of both shoulders and right stifle joint – Right shoulder:
The volume, echogenicity and echotexture of both the supra- and infraspinatus muscle
are within normal limits.
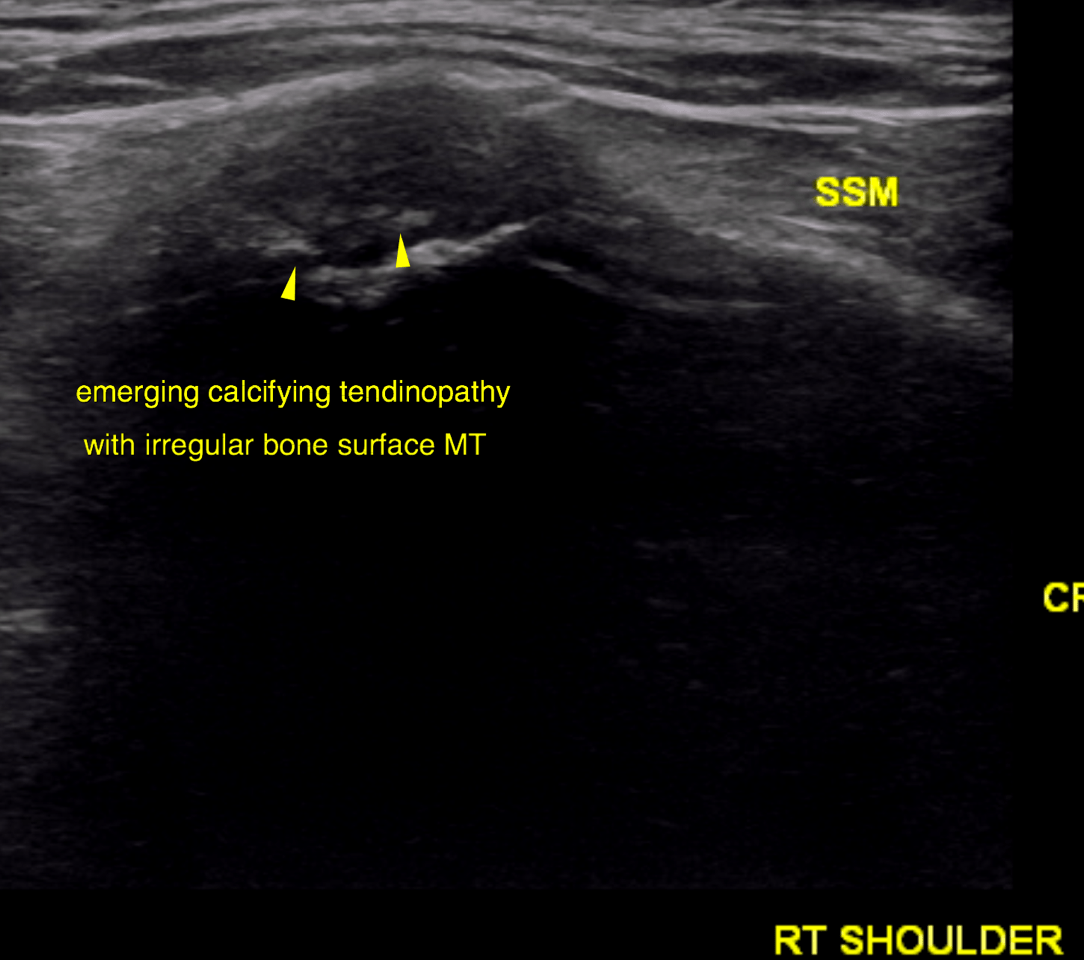
The distal insertion tendon of the supraspinatus appears to be normal in volume; there
is no impingement on the biceps tendon noted. Several foci of emerging calcification
are noted next to the slightly irregular bone surface of the major humeral tubercle.
The distal insertion tendon of the infraspinatus is even in width, smooth in outline and
presents a regular fibre pattern. The attachment to the bone is within normal limits.
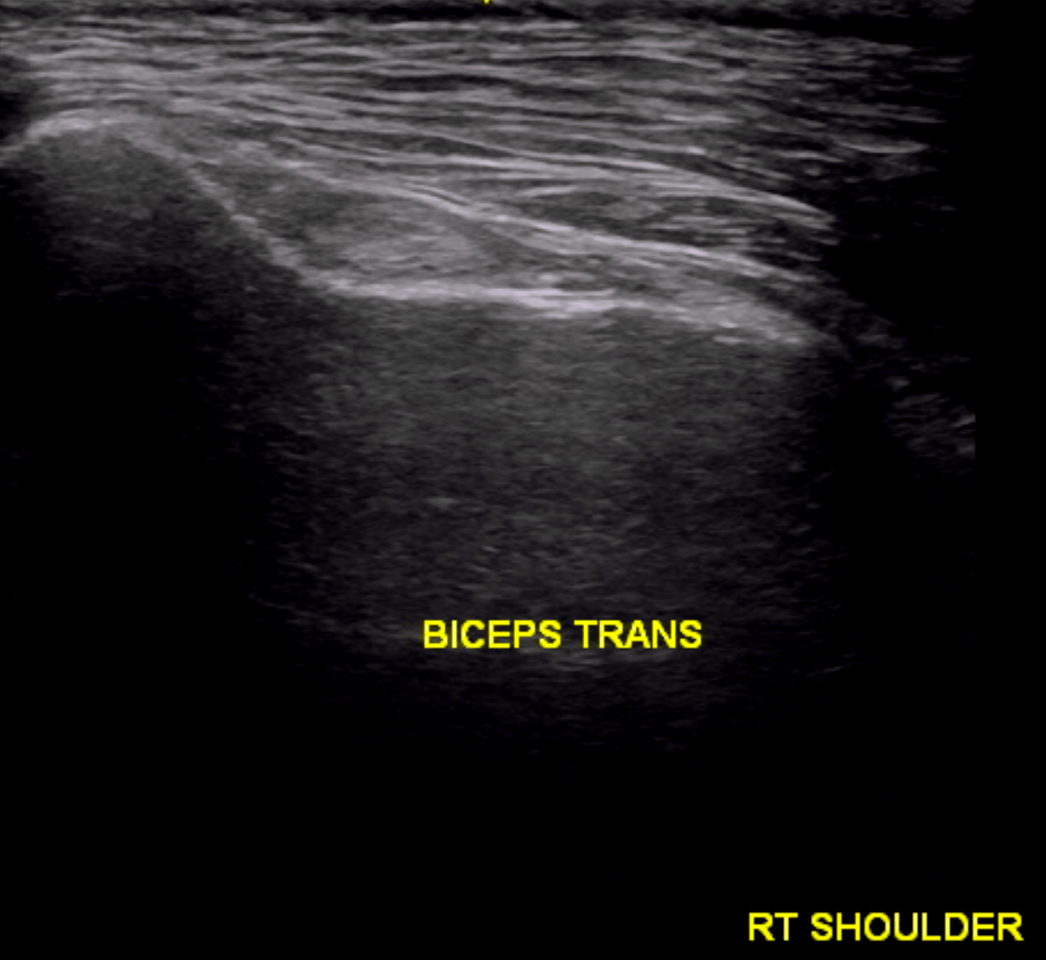
The biceps tendon is even in width, smooth in outline and presents a regular and
uniform fibre pattern. There is no tendon sheath effusion or thickening. The bone
surface of the intertubercular groove is even and smooth.
Left shoulder:
The volume, echogenicity and echotexture of both the supra- and infraspinatus muscle
are within normal limits.
The distal insertion tendon of the supraspinatus appears to be normal in volume; there
is no impingement on the biceps tendon noted. The echoarchitecture of the tendinous
attachment to the major humeral tubercle is within normal limits. The bone surface is
even and smooth. The distal insertion tendon of the infraspinatus is even in width, smooth in outline and
presents a regular fibre pattern. The attachment to the bone is within normal limits.
The biceps tendon is even in width, smooth in outline and presents a regular and
uniform fibre pattern. There is no tendon sheath effusion or thickening. The bone
surface of the intertubercular groove is even and smooth.
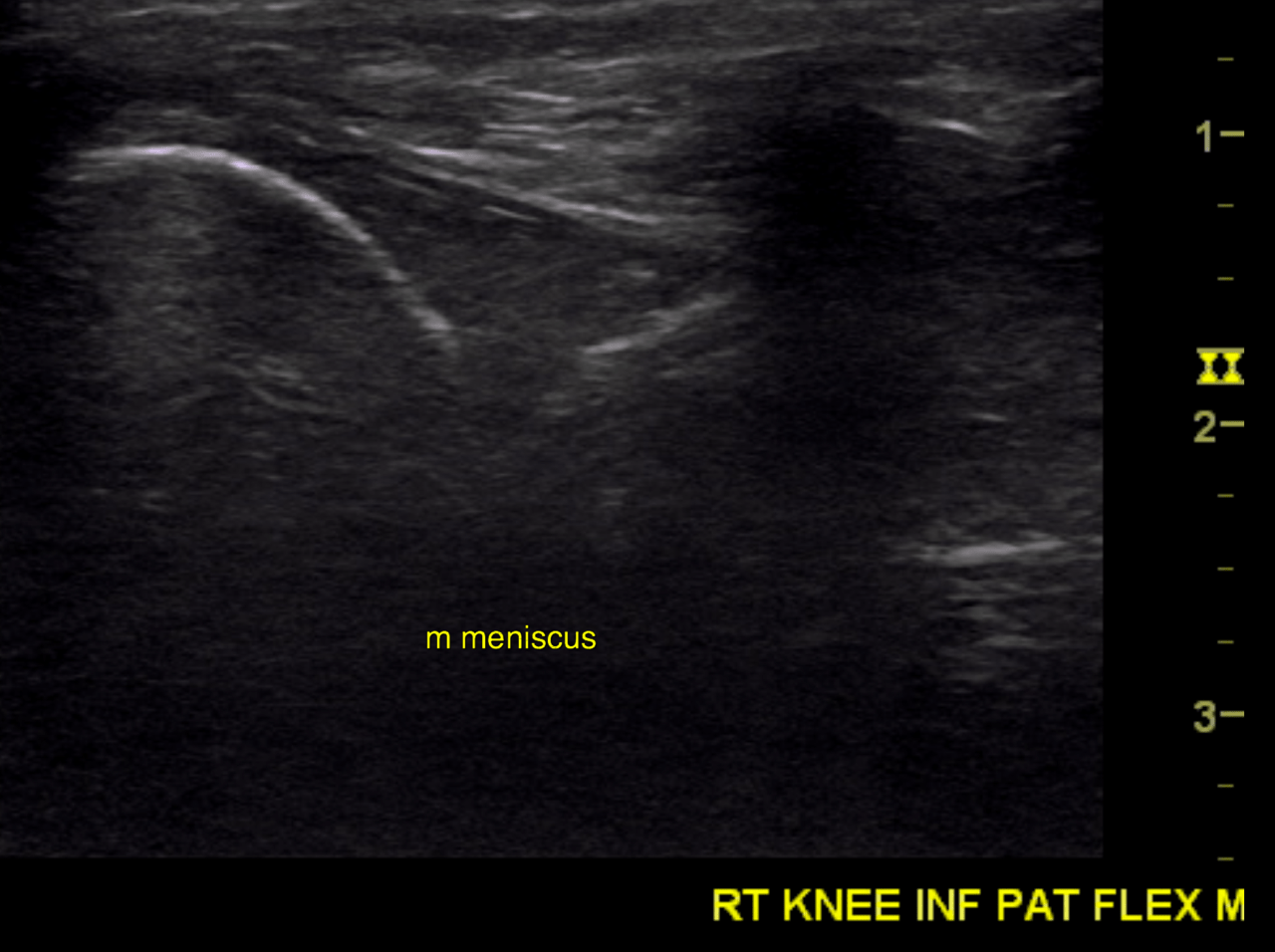
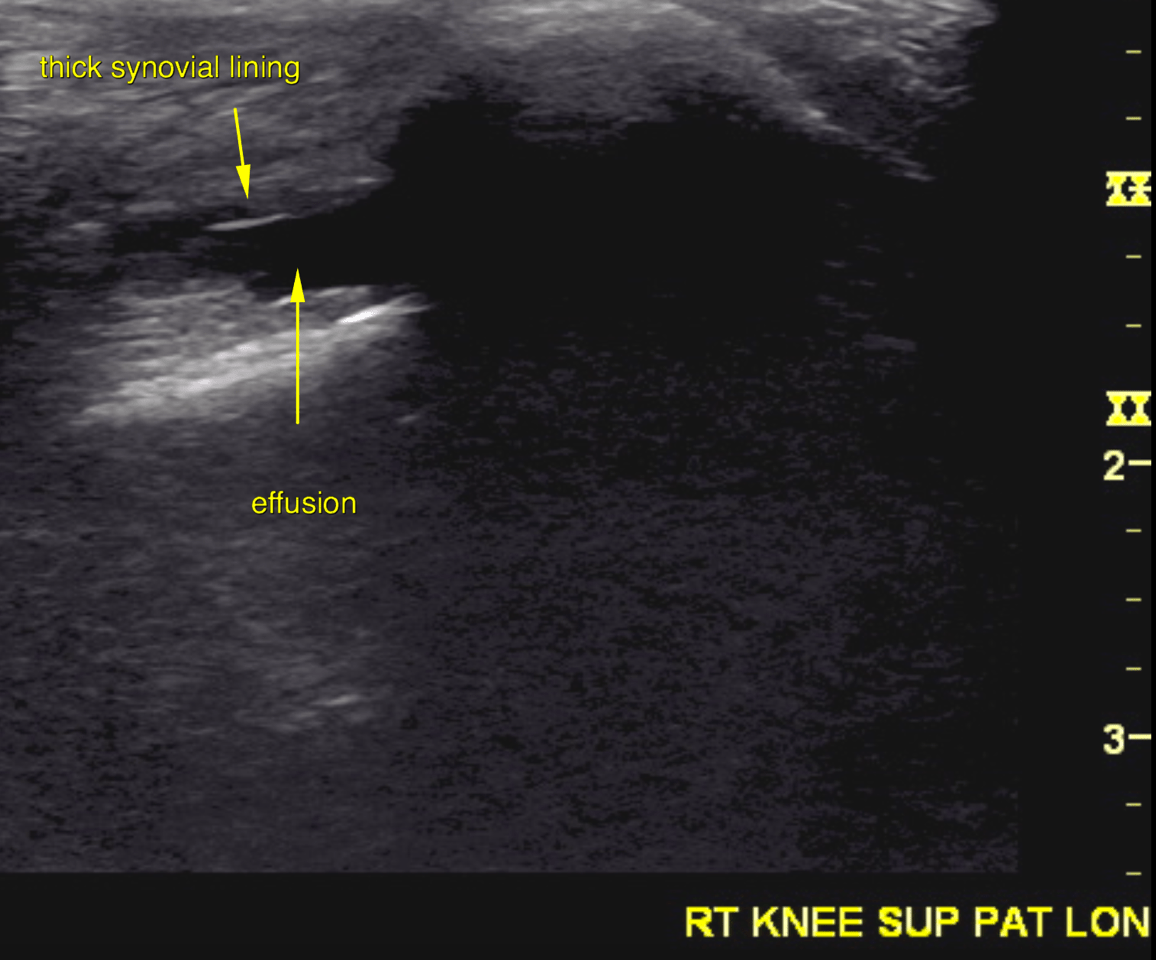
Right stifle:
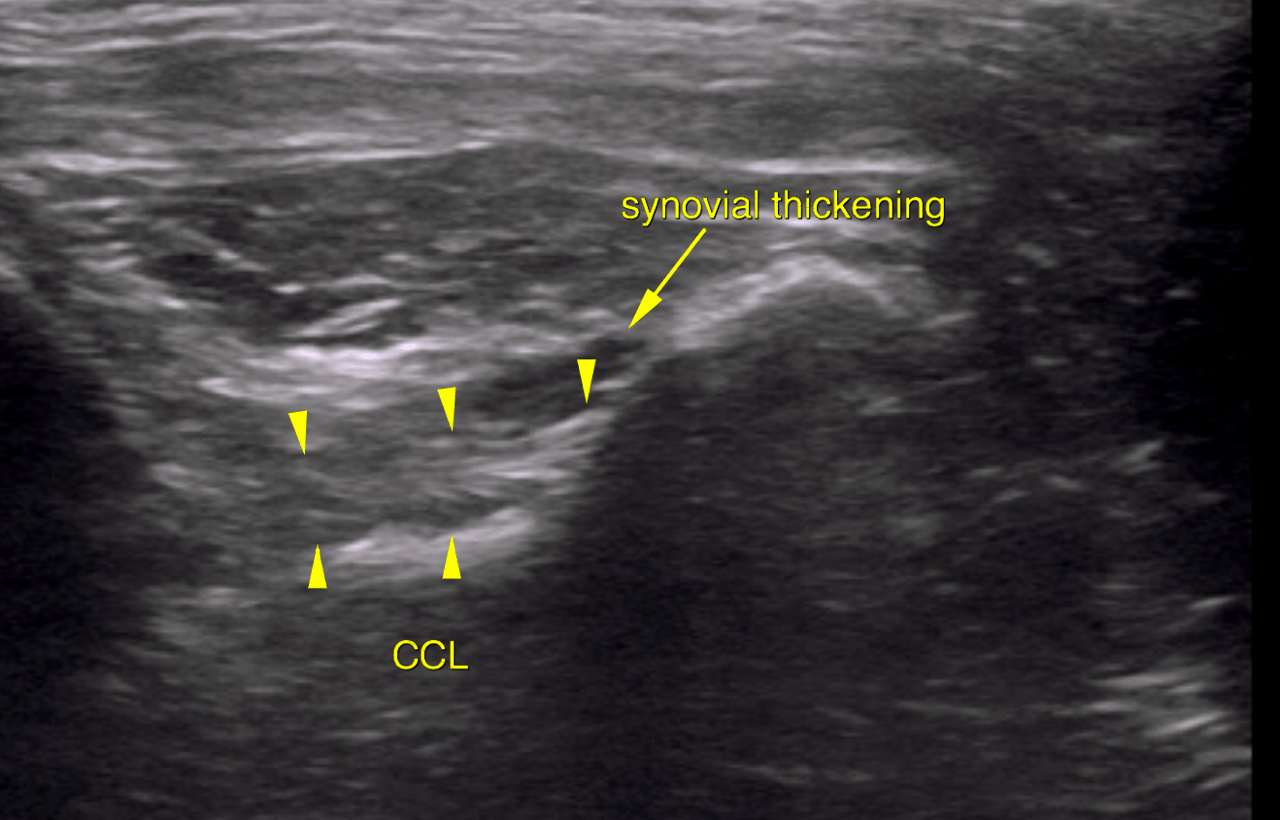
A mild amount of anechoic effusion and mild synovial thickening is noted within the
suprapatellar recess of the right stifle joint.
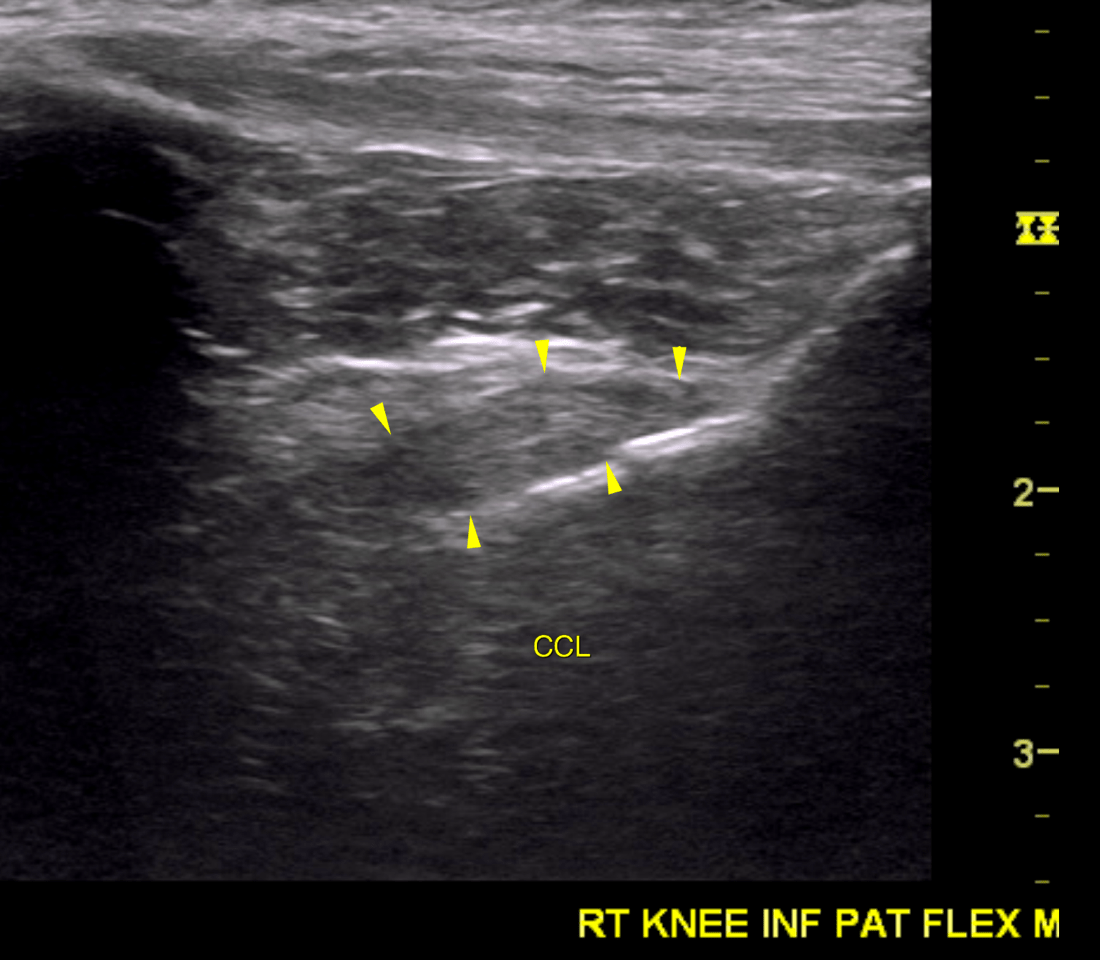
The infrapatellar recess is devoid of effusion and scant synovial thickening is noted.
The infrapatellar fat pad presents with the expected regular echoarchitecture.
The cranial cruciate ligament is continuous with a regular fibre pattern, even thickness
and smooth outline.
The medial meniscus is in situ, uniform in echogenicity and smooth in outline. The
lateral meniscus reveals very few non-shadowing echogenic foci, but is in situ with
uniform echogenicity and smooth outline.
The ultrasonographic do not support a musculotendinopathy in the left shoulder as
underlying cause of the current clinical presentation.
There is no evidence of direct or indirect (mechanical impingement on biceps tendon)
clinical significance of the emerging calcifying tendinopathy of the right supraspinatus.
Even though the ultrasonographic examination of the right stifle joint supports the
presence of mild chronic degenerative joint disease there is no evidence of cranial
cruciate or meniscal pathology at this point. Consider other arthropathy such as
immune mediated arthritis as differential diagnosis and consider aspiration of synovia
should the ultrasonographic findings not parallel the clinical presentation. The findings
do neither support infectious or other erosive arthritis nor a recent hemarthros.