A 14-year-old FS Bengal cat with history of polycystic kidneys was presented for hematuria. Physical exam was unremarkable. Blood chemistry revealed slight hyperamylasemia. CBC was within normal limits. In-house urinalysis showed normal pH, specific gravity and a full field of RBCs on microscopic evaluation. Patient was presented several weeks later for vocal changes, including loss of voice, accompanied by wheezing. Physical exam at that time found the patient to be febrile. Her throat palpated normally. Blood chemistry revealed only high triglycerides.
A 14-year-old FS Bengal cat with history of polycystic kidneys was presented for hematuria. Physical exam was unremarkable. Blood chemistry revealed slight hyperamylasemia. CBC was within normal limits. In-house urinalysis showed normal pH, specific gravity and a full field of RBCs on microscopic evaluation. Patient was presented several weeks later for vocal changes, including loss of voice, accompanied by wheezing. Physical exam at that time found the patient to be febrile. Her throat palpated normally. Blood chemistry revealed only high triglycerides. CBC found leukocytosis and neutrophilia. T4 was within normal range. Urinalysis showed normal pH and specific gravity, a turbid red appearance, proteinuria (3+), hematuria (3+), WBC (4-10), RBC (51-100), and moderate amorphous debris. Urine microalbumin was high. Urine culture yielded no growth. Antibiotic injection and subcutaneous fluids were given, and patient was discharged. Upon recheck exam a few days later, patient was BAR, with slightly tacky mucous membranes, prominent kidneys, mild ocular discharge, heart and lungs clear with no overt murmurs or wheezes ausculted. Thoracic radiographs showed no abnormalities. Patient received subcutaneous fluids, an antibiotic injection, and was referred for ultrasound.
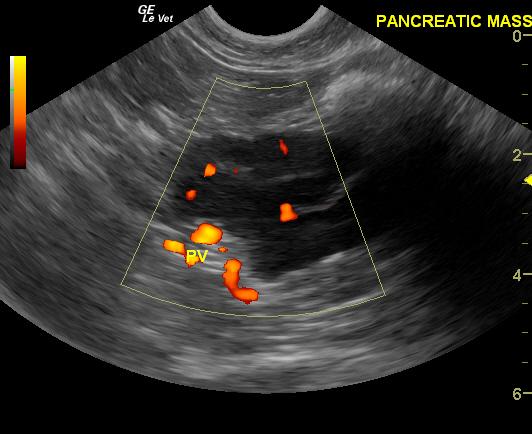
Pancreatic adenoma in a 14 year old FS Bengal cat
History
Comments
A good prognosis was given. Surgical removal of the mass was not recommended, although if it increased in size could lead to possible bile duct obstruction.
Clinical Differential Diagnosis
Hematuria – pyelonephritis, renal hemorrhage, low grade urinary tract infection, cystitis, cystic calculi, urinary bladder neoplasia, polycystic kidneys. Hyperamylasemia – decreased renal clearance, intestinal inflammation (IBD), pancreatitis.
DX
Sampling
A coagulation panel revealed PT of 18 seconds and PTT that was slightly elevated (biopsy was not clinically contraindicated). An 18 gauge ultrasound guided Tru-cut® biopsy was performed of the pancreatic lesion. Biopsy results taken from the pancreatic mass revealed a pancreatic adenoma consisting of acinar cells.
Sonographic Differential Diagnosis
Pancreatic mass, possible pancreatic carcinoma or lymphoma, possible sequestrum or necrosis. Ultrasound guided biopsy performed.
Image Interpretation
A 2.5 x 4.4cm pancreatic mass was present which occupied the pancreatic base and extended over to the right limb through the portal vein. The mass could also be seen in minimal portions of the left limb. This is highly suggestive for infiltrative disease such as pancreatic lymphoma or carcinoma, however pancreatic sequestrum is also a possibility.
Outcome
Owner was advised to have follow-up ultrasound performed if patient became icteric.
Video
Patient Information
Blood Chemistry
- Amylase, High
- Hypertriglyceridemia
CBC
- Neutrophils, High
- WBC, High
Clinical Signs
- Hematuria
- Voice changes
- Wheezing
History
- Polycystic kidneys
Exam Finding
- Dehydration
- Fever
- Large Kidneys
- Ocular Discharge
Urinalysi
- Albumin Present
- Appearance Turbid
- Blood Present
- Protein Present
- WBCs Present
Images