12-year-old MN DSH with a history uncontrolled diabetes mellitus was presented for evaluation of ravenous appetite, shaking, and restlessness. Current therapy was 9 IU PZI SQ BID. Urinalysis showed SG of 1.024 and glycosuria. CBC was within reference range. Abnormalities on serum biochemistry were hyperglycemia, elevated ALT and ALP activity, and hypokalemia. T4 was within reference range.
12-year-old MN DSH with a history uncontrolled diabetes mellitus was presented for evaluation of ravenous appetite, shaking, and restlessness. Current therapy was 9 IU PZI SQ BID. Urinalysis showed SG of 1.024 and glycosuria. CBC was within reference range. Abnormalities on serum biochemistry were hyperglycemia, elevated ALT and ALP activity, and hypokalemia. T4 was within reference range.
Poor glycemic control – owner compliance (administration, diet), insulin bottle (expired, incorrect storage)
Incorrect insulin
Somogyi overswing
Insulin resistance – Cushing’s disease, insulin antibodies
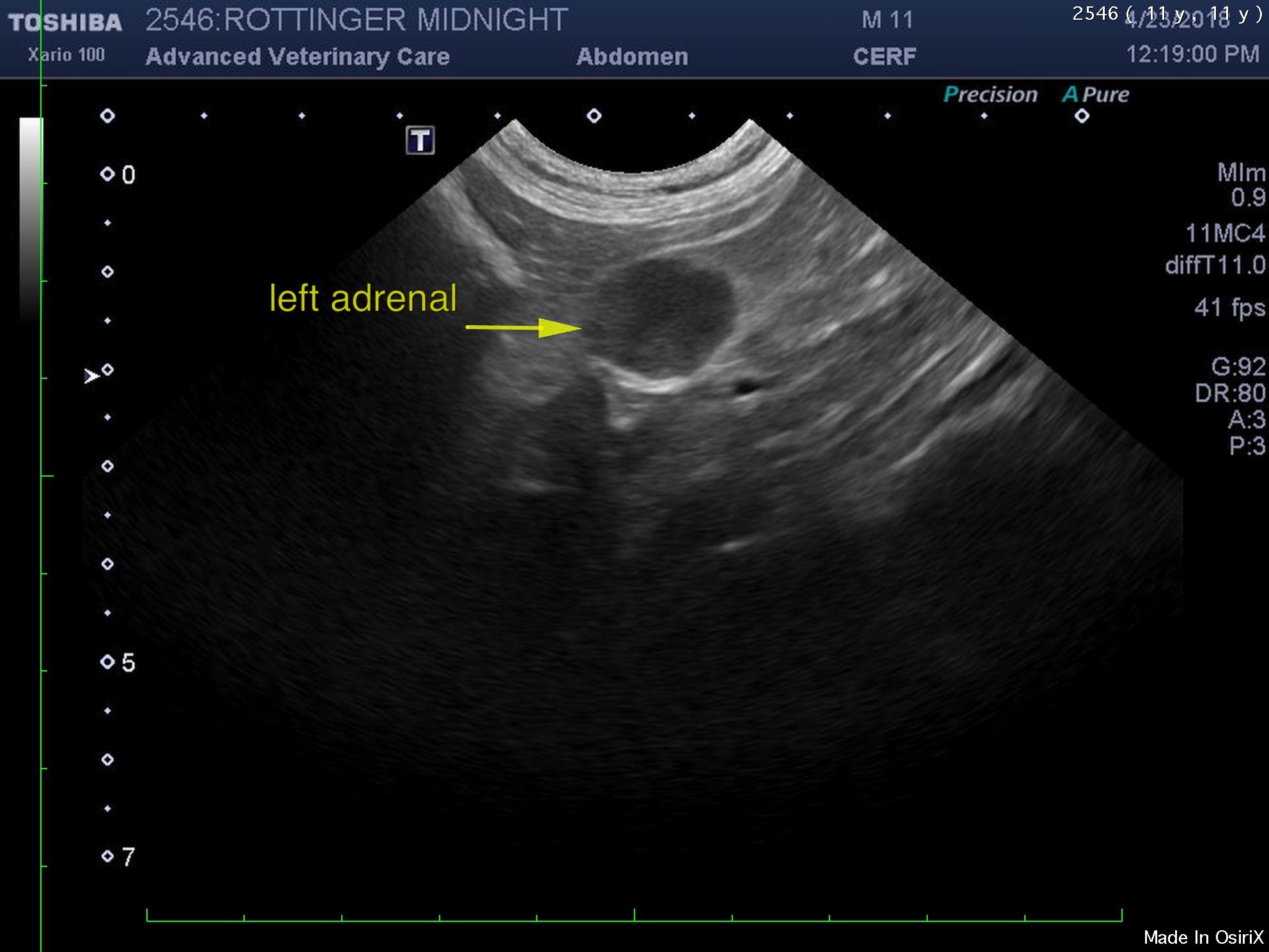
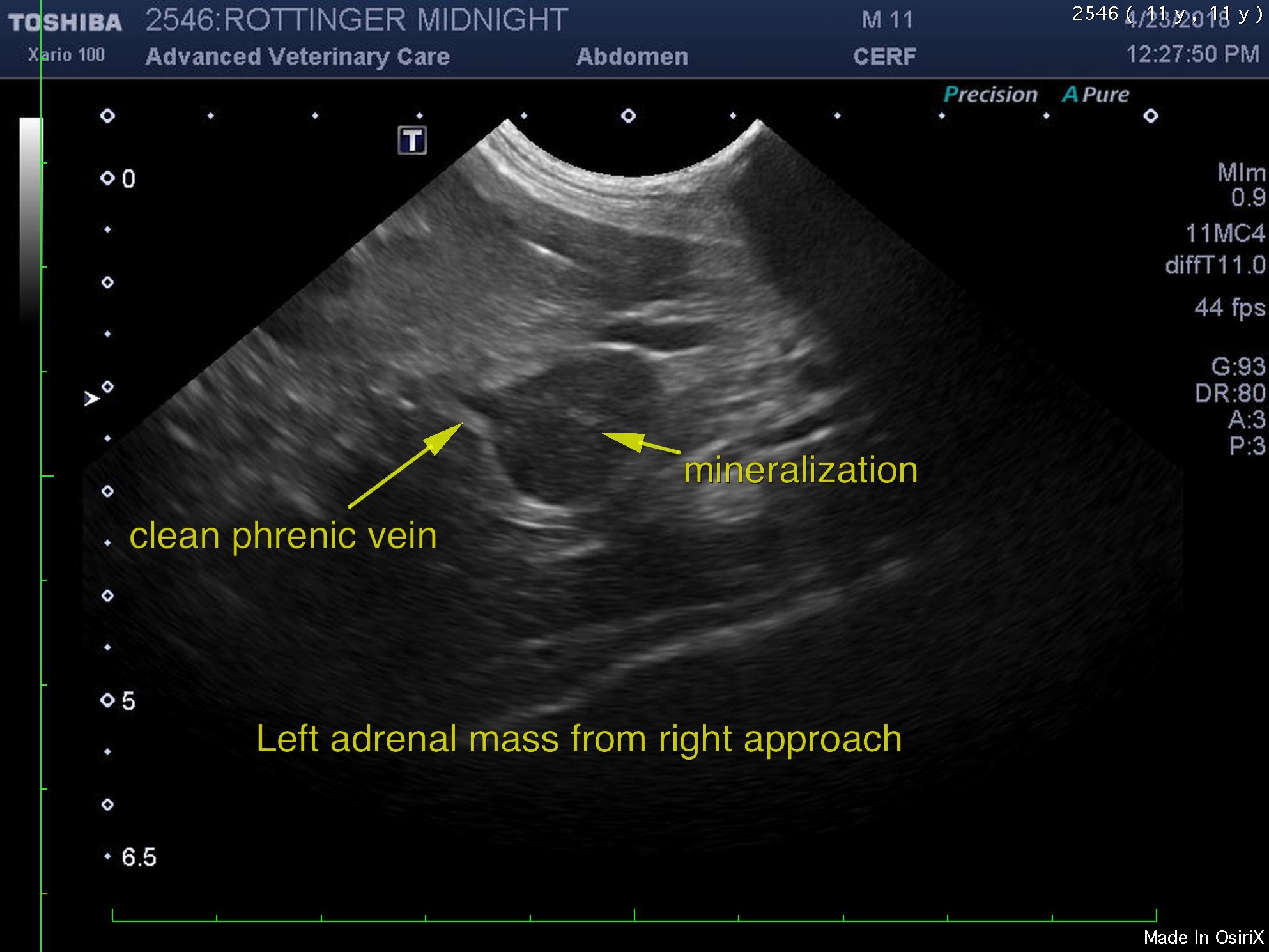
The left adrenal gland was enlarged in this patient and hypoechoic. The left adrenal revealed focal mineralization with no evidence of vascular invasion. The left adrenal measured 1.5 cm with capsular expansion without capsular escape. The right adrenal gland was uniform and subnormal in size. The right adrenal gland was isoechoic to the surrounding fat.
I recommend assessment of sodium potassium ratios in this patient to assess for Conn’s syndrome as well as testing for functional left adrenal adenocarcinoma. This appears resectable. Surgical resection is recommended. Blood pressure measurements would be warranted. LDDST at 0.1 mg/kg induction is recommended.