Dr. Karen Ebersole, owner of Scanvet, a mobile veterinary ultrasound service in Auburn, Maine submitted this rather brilliant feline VSD case after attending SonoPath’s SDEP™ ECHO course this past March. She selected our SonoPodcast option for this echocardiogram where Dr. Eric Lindquist offers his critique of technique on submitted ultrasound scans, plus a report. You can use these valuable videos with voiceover to further educate yourself on scanning approaches and angles to increase your own ultrasound efficiency. To submit a SonoPodcast, select it from the drop down menu on SonoPath’s SPA: Your Home for Educational Telemedicine™
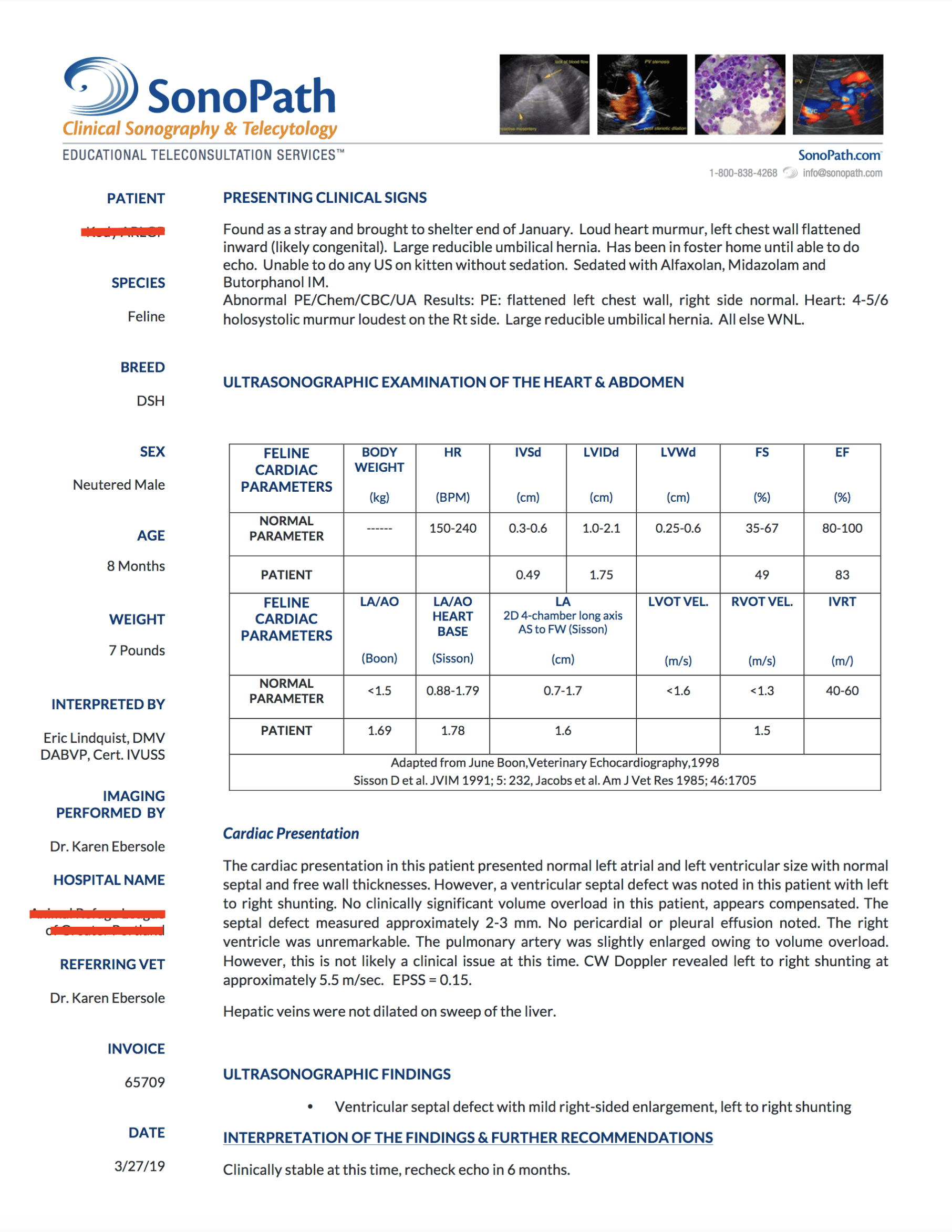
The patient was found as a stray. Loud heart murmur, left chest wall flattened inward (likely congenital). Large reducible umbilical hernia. Unable to do any ultrasound on kitten without sedation. Sedated with Alfaxolan, Midazolam and Butorphanol IM. Physical exam: flattened left chest wall, right side normal. Heart: 4-5/6 holosystolic murmur loudest on the Rt side. Large reducible umbilical hernia, all else WNL.
The patient was found as a stray. Loud heart murmur, left chest wall flattened inward (likely congenital). Large reducible umbilical hernia. Unable to do any ultrasound on kitten without sedation. Sedated with Alfaxolan, Midazolam and Butorphanol IM. Physical exam: flattened left chest wall, right side normal. Heart: 4-5/6 holosystolic murmur loudest on the Rt side. Large reducible umbilical hernia, all else WNL.
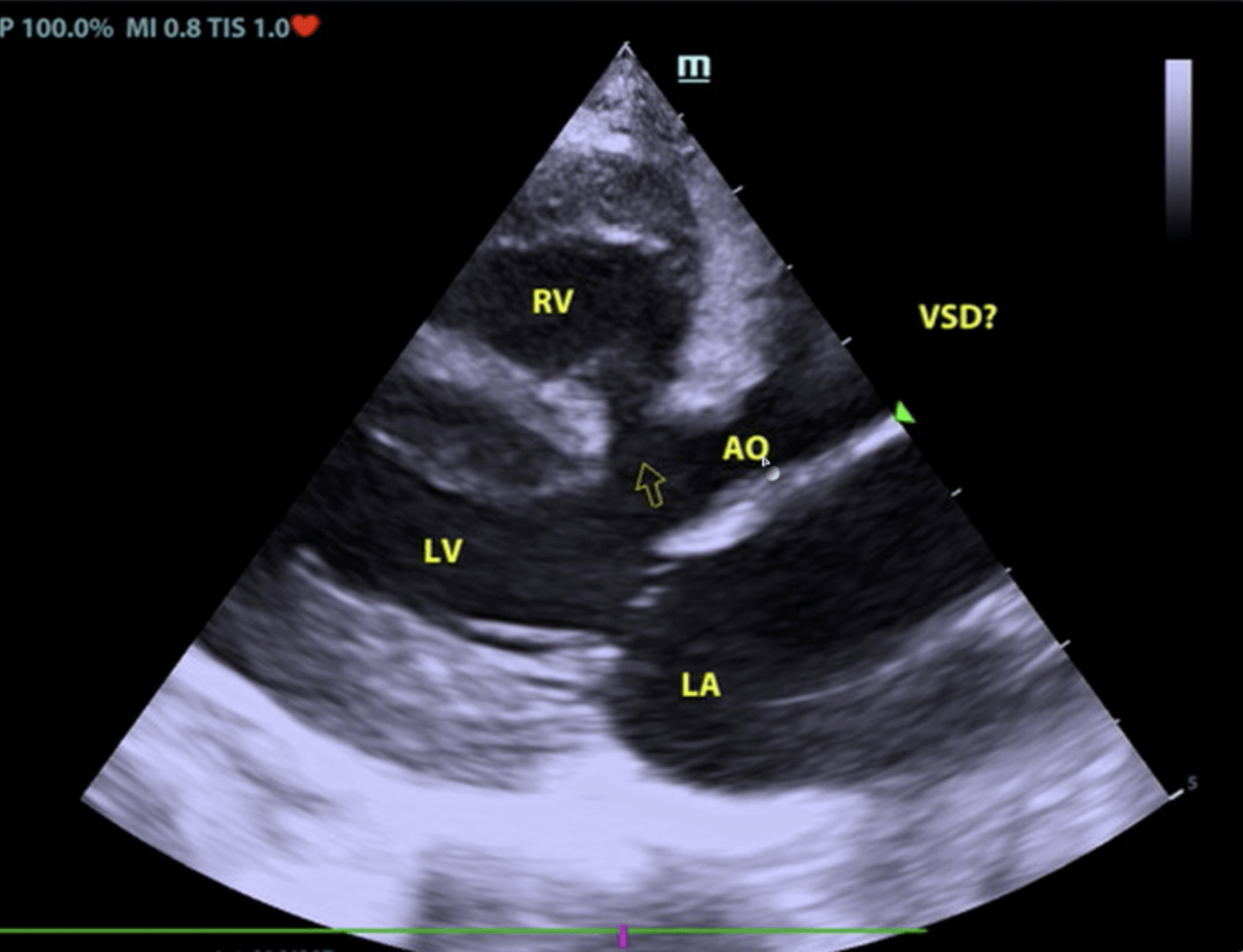
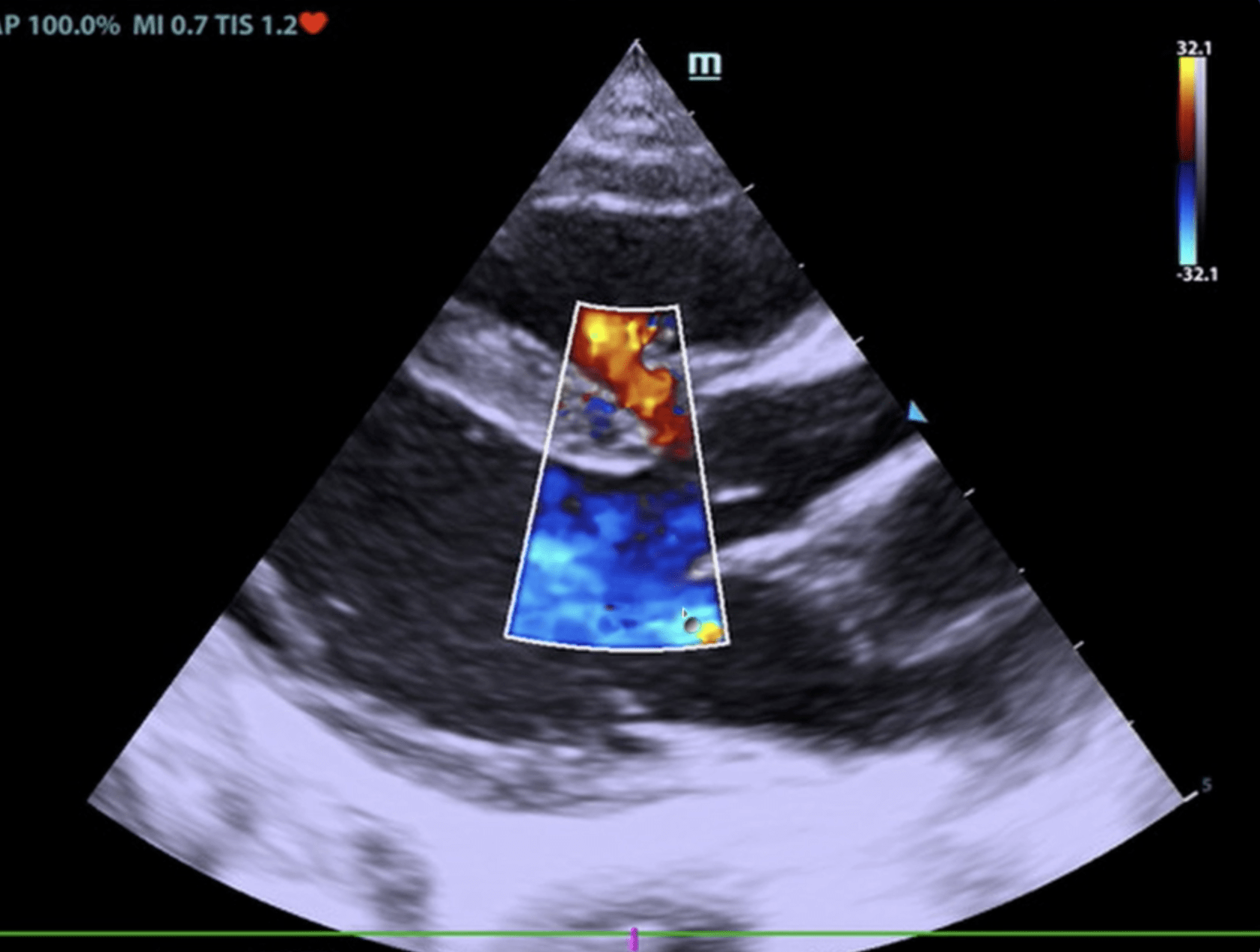
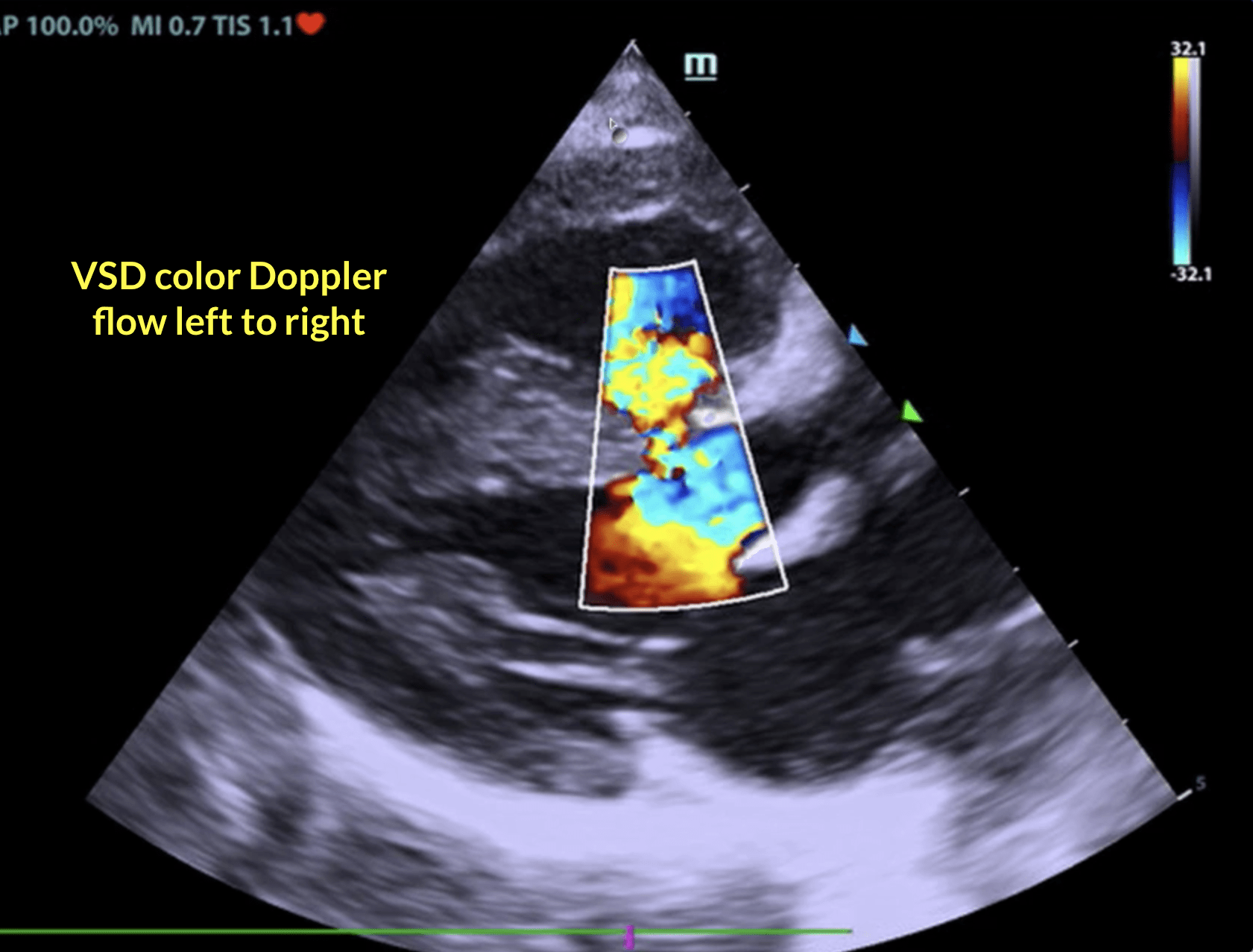
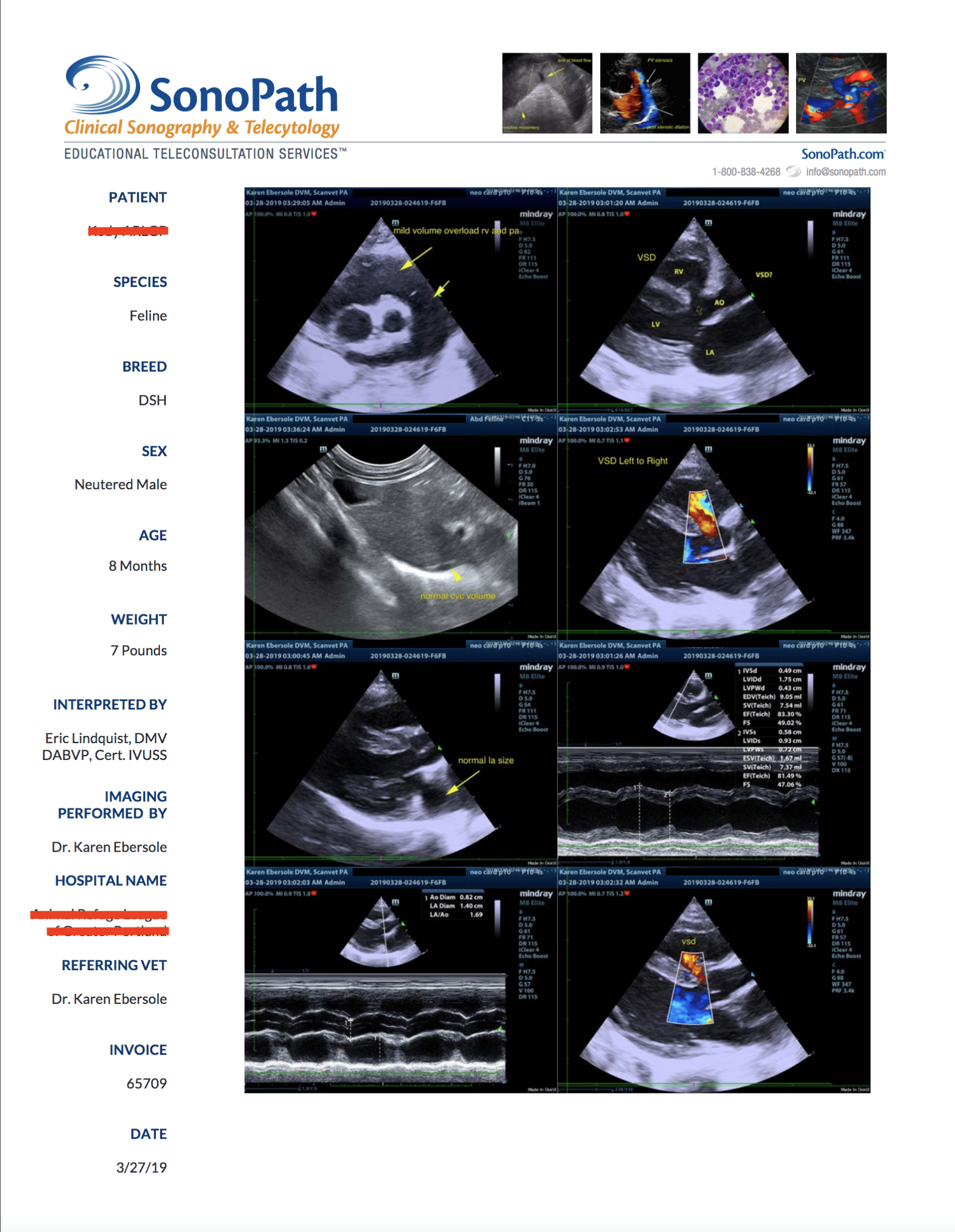
Ventricular septal defect with mild right-sided enlargement, left to right shunting.
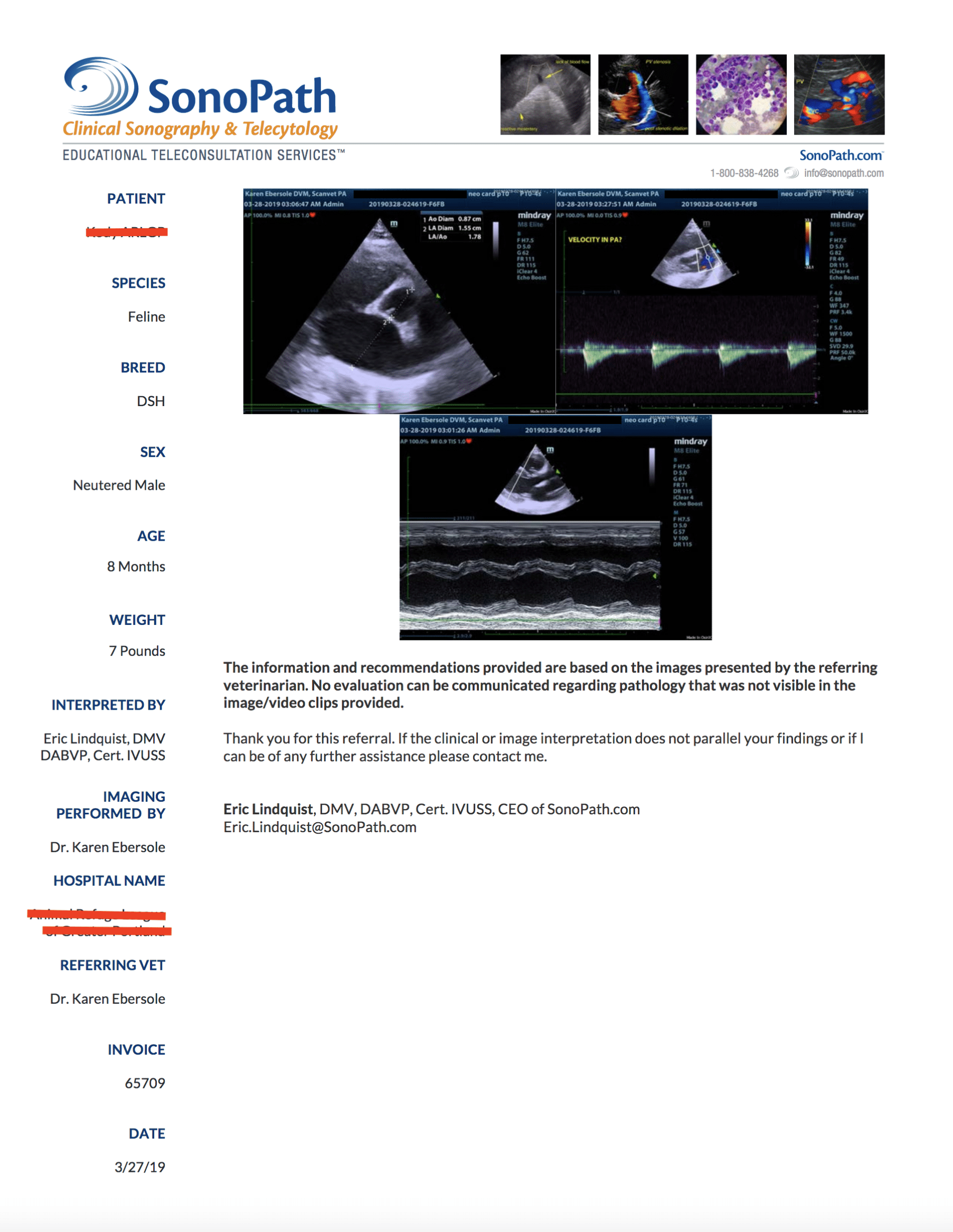
A ventricular septal defect was noted in this patient with left to right shunting. No clinically significant volume overload, appears compensated. The septal defect measured approximately 2-3 mm. CW Doppler revealed left to right shunting at approximately 5.5 m/sec.
Additional cardiac information: the heart presented normal left atrial and left ventricular size with normal septal and free wall thicknesses. No clinically significant volume overload in this patient, appears compensated. No pericardial or pleural effusion noted. The right ventricle was unremarkable. The pulmonary artery was slightly enlarged owing to volume overload. However, this is not likely a clinical issue at this time. Hepatic veins were not dilated on sweep of the liver. Interpretation of the Findings & Further Recommendations: Clinically stable at this time, recheck echo in 6 months.