Sam-I-Am! Ever want to know how to dissect out an HCM heart sonographically regarding hypertrophy, dynamic outflow obstruction (SAM), bidirectional turbulence and decide if clinical or not? Our SonoPath Cardiologist Maggie Machen DACVIM (Cardiology) demonstrates Educational TelemedicineTM artistry in her evaluation of the cat heart imaged by Andi Parkinson RDMS of Intrapet Imaging, Baltimore, MD, USA in the October, 2016 SonoPath Educational TelemedicineTM case of the month. Want to start or improve your echocardiogram game? We have made it step by step simple for you with our program taught successfully to hundreds of veterinary sonographers over the years; with a simple twist or a tilt or a push you can get the views you need every day.
Check out our educational products for rock star echocardiogram imaging with the SDEP downloadable cardiac program https://sonopath.com/products/downloadable
SDEP Poster:
https://sonopath.com/products/poster
Normals DVD abdomen and Cardiac with efficiency clips to obtain the rapid normal images in a short amount of time with 3 second maneuvers:
https://sonopath.com/products/cd
& of course our SDEP echo seminar this November 18-20, 2016 in Sarasota, Florida with Mandi Klemen DACVIM (Cardiology)
http://sonopath.com/events/2016-sdep-ce-events/nov-18-20-sdep-echo-sarasota-fl
A 10-year-old, FS, DSH cat was presented for assessment of murmur and anesthetic risk prior to dental prophylaxis. An exam 1-month prior revealed a grade III/VI murmur. NT-proBNP was >1500pmol/L. The patient was on no medications at the time of ultrasound. CBC/Chem/UA were all WNL. Radiographs showed cardiomegaly.
A 10-year-old, FS, DSH cat was presented for assessment of murmur and anesthetic risk prior to dental prophylaxis. An exam 1-month prior revealed a grade III/VI murmur. NT-proBNP was >1500pmol/L. The patient was on no medications at the time of ultrasound. CBC/Chem/UA were all WNL. Radiographs showed cardiomegaly.
Hypertrophic obstructive cardiomyopathy.
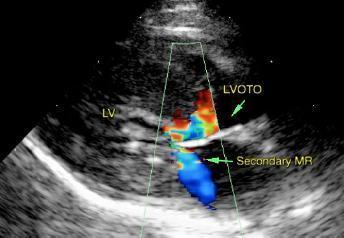
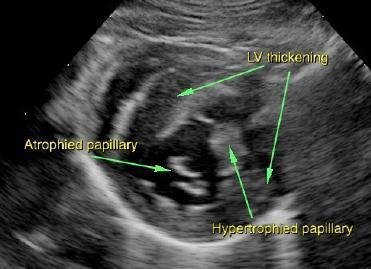
The left ventricular wall is moderate to severely asymmetrically hypertrophied. There is a diffusely hyperechoic endocardium consistent with fibrosis and ventricular remodeling. Asymmetric papillary muscle hypertrophy and atrophy. The right ventricle is subjectively normal in size and morphology. There is mild left atrial enlargement present. No right atrial enlargement present. Elevated RVOT velocity consistent with a dynamic obstruction. There is mild to moderate systolic anterior motion (SAM) of the mitral valve present, with a mildly elevated LVOT velocity. There is moderate eccentric mitral regurgitation present secondary to SAM. No other obvious valvular regurgitation is present. There is no pericardial effusion noted. No pleural effusion appreciated.
This indicates LV hypertrophy with a dynamic LVOT obstruction (SAM). There is mild left atrial dilation, indicating the risk of a future spontaneous CHF and/or a thrombotic event may be elevated. There is also a benign RV outflow obstruction (DRVOTO). If able, administer titrating dose of atenolol: 2.5mg tablets; Give tab once daily. Recheck heart rate in 1-2 weeks with target stressed rate of 140-160bpm 12-24 hours post administration. Increase as needed until target reached. Screening blood pressure is recommended. Recommend recheck echocardiogram in 6 months to assess for progression, sooner if clinical issues arise.