“What Does This?” The ubiquitous question we all ask ourselves when a clinical presentation walks through our door. In the northeast rainstorms come through and here comes the Lepto caseload 3-7 days later like a shadow behind the storm. Come see what Pennsylvania Mobile sonographer Rebekah Jakum RVT/RVT (http://www.pamobile.net/) found on this geriatric Aussie successfully managed by the staff at Rossmoyne Veterinary Emergency Center in Harrisburgh, PA (http://raetc.com/).
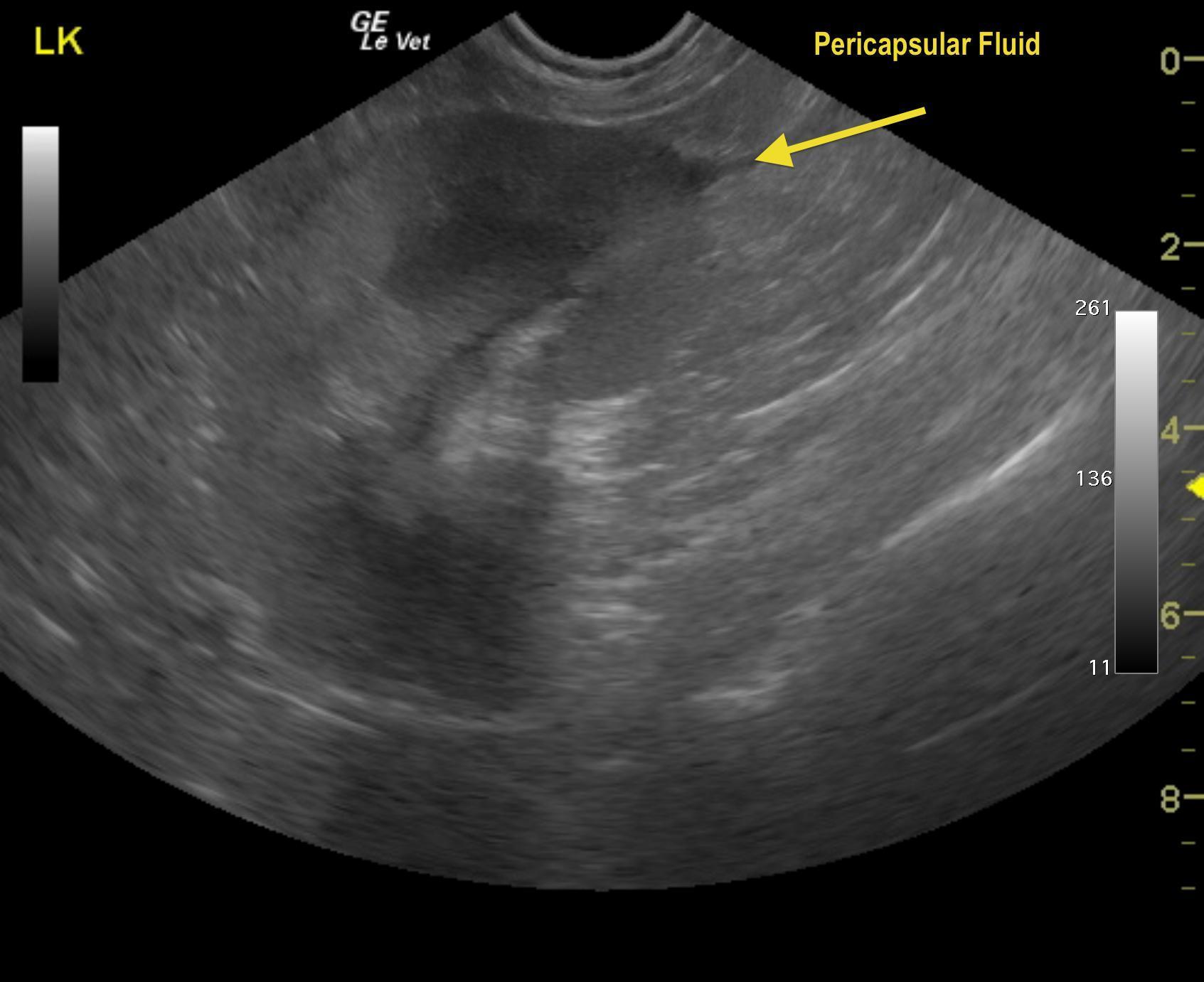
Lepto cases can present with a rapid onset of “ADR,” renal +/- liver failure and a particular sonographic renal presentation that may be structurally normal owing to acute insult. Or, the kidneys may present in this manner shown here with mild archotectural distortion and pericapsular fluid formation. Or, in chronic cases, a chronic interstitial pattern may be present. Do a basic search on sonopath on your Iphone or Android App or through the site and see what we see from the inside out (http://sonopath.com/members/case-studies/search?text=leptospirosis&species=All).
A 13-year-old MN Border Collie was presented for anorexia. Blood chemistry revealed moderate to severe BUN, creatinine and phosphorus with minor ALT, CPK and globulin elevations. Urinalysis revealed isosthenuria was present with a urine PH of 6.0 and some epithelial cells. Clinical dehydration and depression was present. Survey abdominal radiographs and CBC were unreremarkable.
A 13-year-old MN Border Collie was presented for anorexia. Blood chemistry revealed moderate to severe BUN, creatinine and phosphorus with minor ALT, CPK and globulin elevations. Urinalysis revealed isosthenuria was present with a urine PH of 6.0 and some epithelial cells. Clinical dehydration and depression was present. Survey abdominal radiographs and CBC were unreremarkable.
Acute kidney injury – toxic, infectious (Leptospira, bacterial nephritis, septicemia), hypoxia, renolith, ureteral obstruction, lymphoma.)
ALT elevation: inflammatory or reactive hepatopathy
Acute nephritis presentation with pericapsular fluid accumulation. Immature gallbladder mucocele. Suspect Leptospirosis or acute renal toxin.
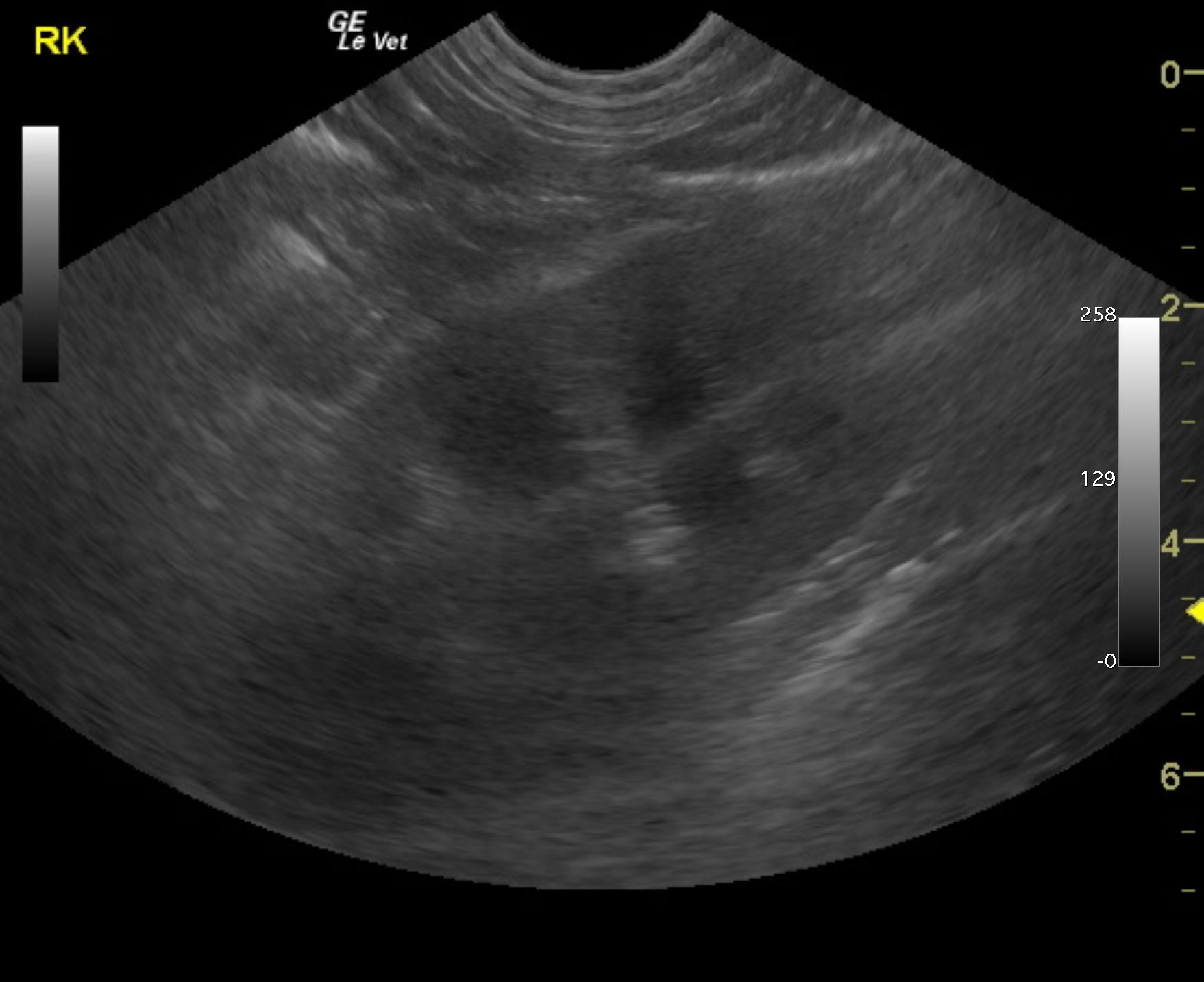
The right kidney presented cortical infarct at the caudal pole. The right kidney measured 7.06 cm.
The left kidney measured 6.97 cm. Pericapsular fluid pattern was noted around both kidneys (more evident on left caudal pole) with
disruption of the corticomedullary definition. Slight pyelectasia was noted in the left kidney as well.
Ill defined pericapsular fat was noted primarily around the left kidney indicative of inflammation. . The gallbladder presented suspended debris and double layered wall. The cystic duct was dilated as was the common bile duct at 0.36 cm. This is consistent with immature mucocele. The liver presented a mild increase in the portal markings.