Wait, that’s not supposed to be there…
Working in mobile ultrasound, you just NEVER know what you’re going to see!
January’s Case of the Month had quite an interesting presentation. Imaging was performed by technician Amanda Lacey, SDEP™ Certified Sonographer of Animal Sounds NW in Oregon. Her thoroughness, flexibility and problem-solving skills helped this patient get a quick diagnosis.
When Cardiomegaly is not ‘Cardiomegaly’ what do you do?
After following the SDEP™ Echo 7pt. protocol, go back to the ‘not normal regions’ and image from multiple different angles, put color on it, reposition the pet, and when you are still stumped, you phone a friend.
After checking images on the SonoPath clinical search for suspected hernia, Amanda decided to reach out to SonoPath specialist, Dr. Mac Daniel, DVM, DABVP, for some input on the next best step………an Abdominal Ultrasound.
Taking a look into the abdomen helped put the clinical picture altogether resulting in a diagnosis.
Special thanks to Dr. Yuko Eguchi-Coe of West Hills Animal Hospital, Corvallis, Oregon,for allowing ASNW to be part of this patient’s diagnostic work up.
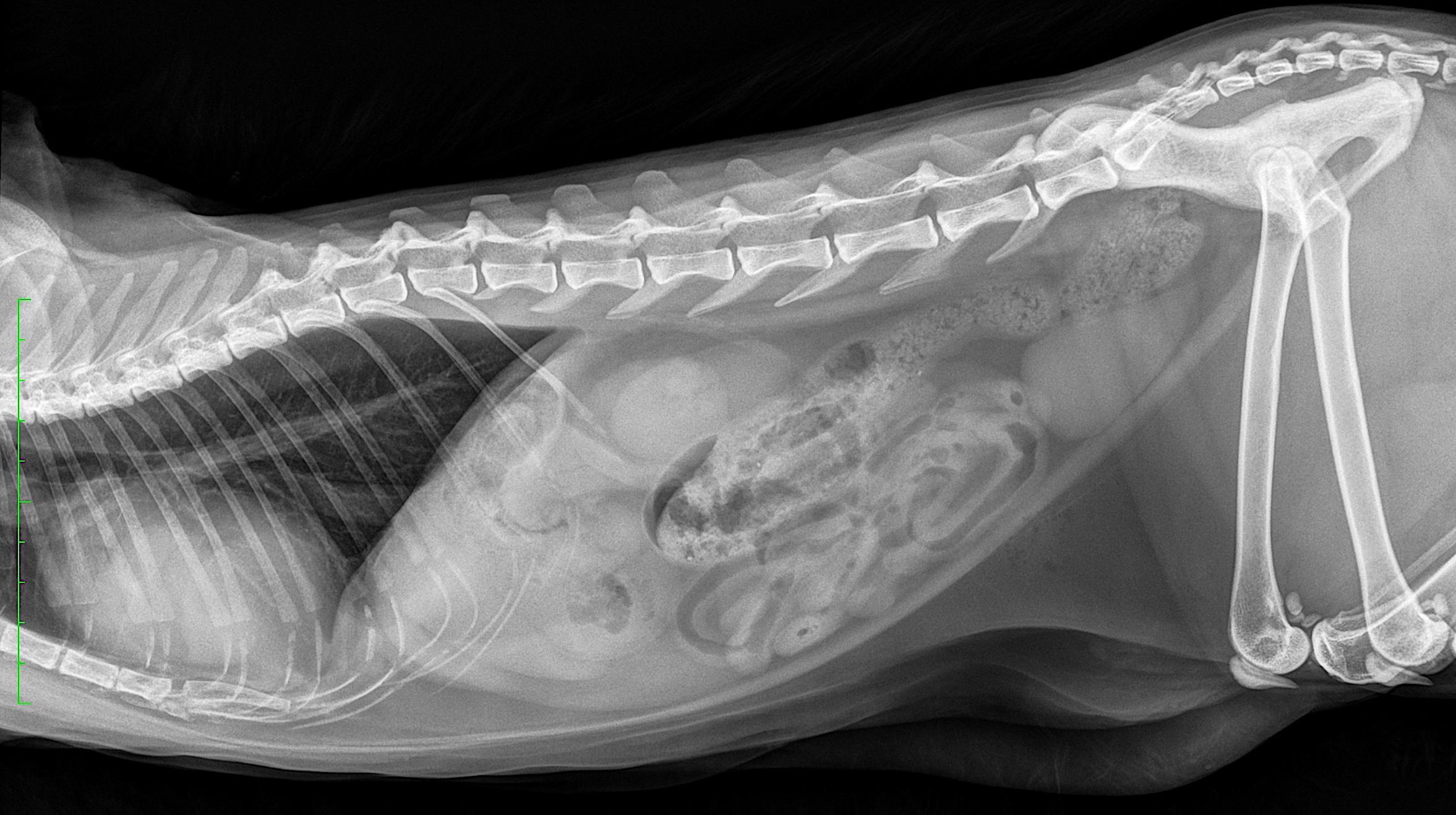
A 2-year-old MN DLH cat presented for lethargy. CBC/Chem/UA showed BUN of 41, urine specific gravity 1.041, 2+ proteinuria, urine culture (+) for Staphylococcus. Generalized cardiomegaly was noted on radiographs in addition to subnormal renal size.
A 2-year-old MN DLH cat presented for lethargy. CBC/Chem/UA showed BUN of 41, urine specific gravity 1.041, 2+ proteinuria, urine culture (+) for Staphylococcus. Generalized cardiomegaly was noted on radiographs in addition to subnormal renal size.
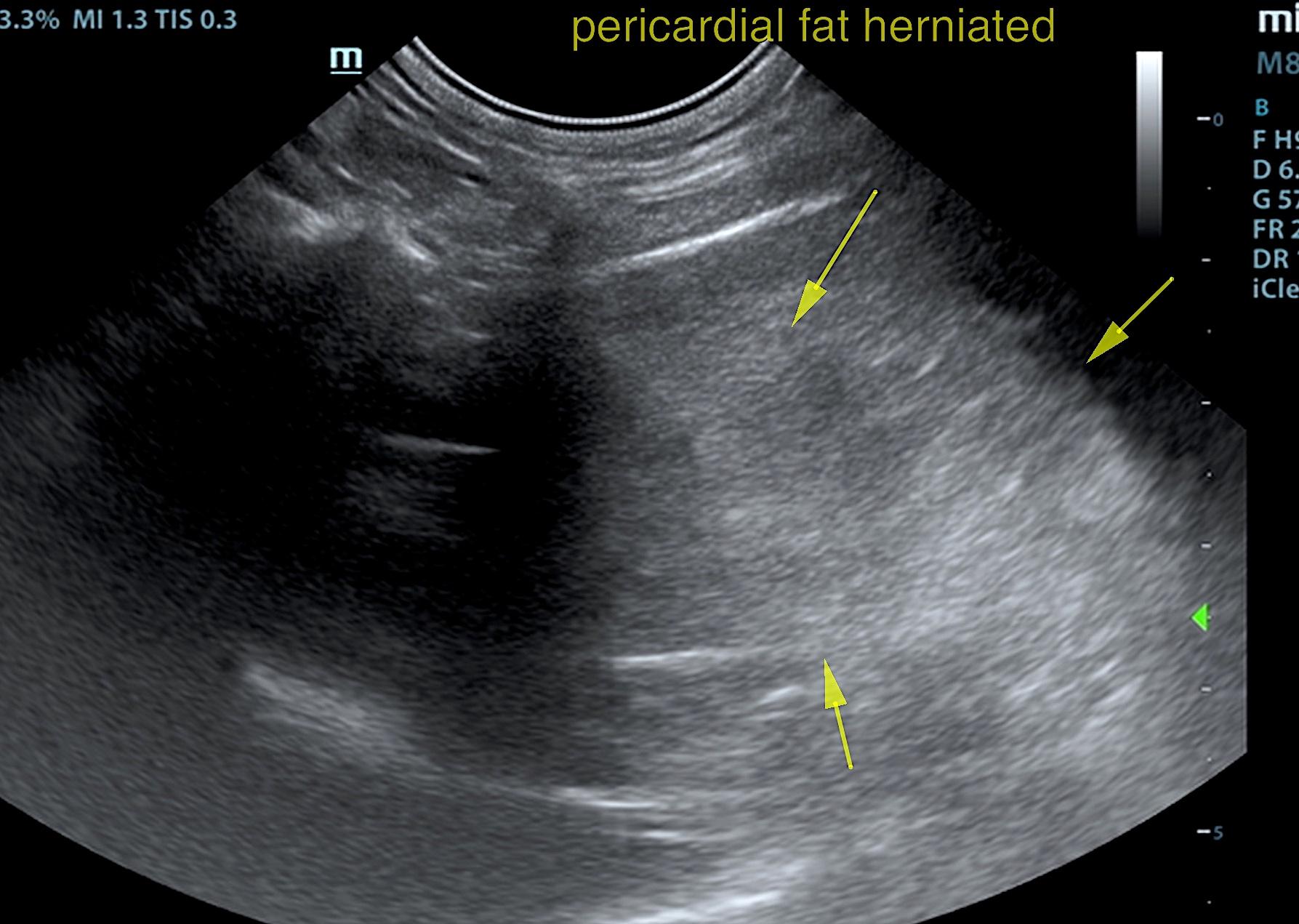
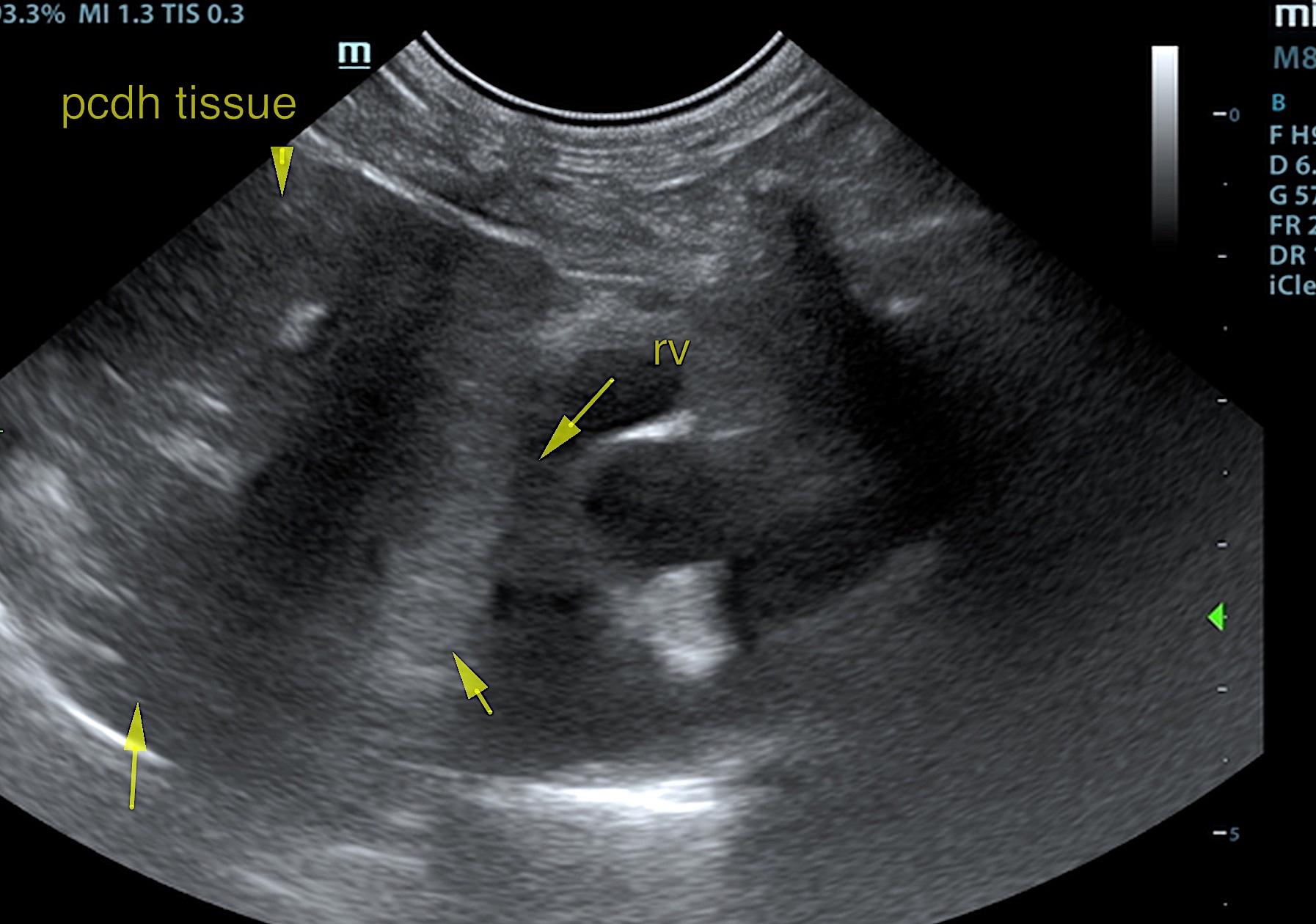
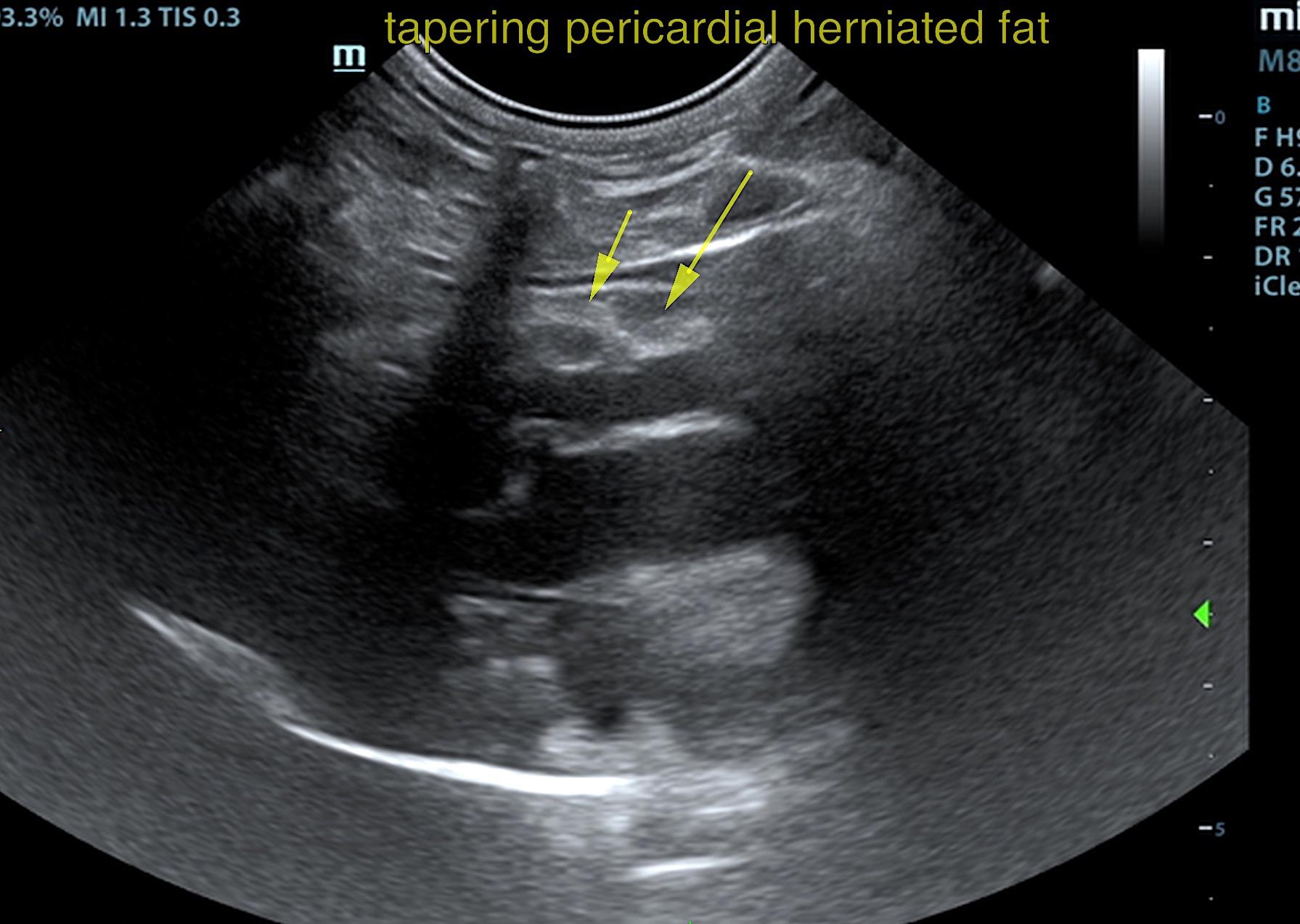
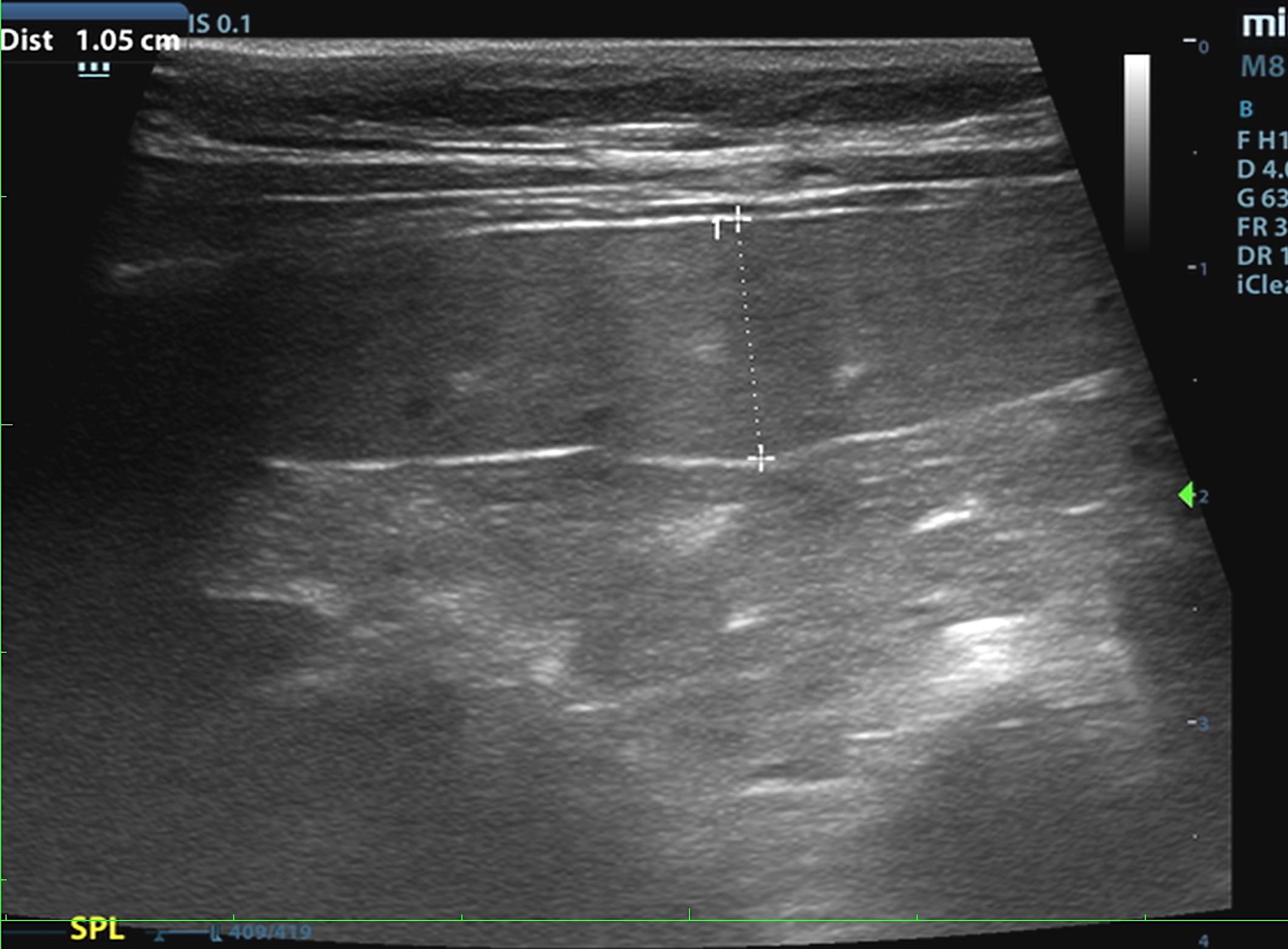
Pericardial diaphragmatic hernia – thoracic herniation of the liver – thoracic and pericardial herniation of the falciform fat. Enlarged spleen.
The spleen was slightly enlarged and mildly irregular measuring 1.44 cm with minor, heterogenous parenchymal changes and scalloping contour. The liver and falciform fat in this patent were displaced cranially as was the stomach. Portions of the liver and falciform fat were herniated through the diaphragm. It appears that mainly fat has entered into the pericardium. However, herniated liver appears to occupy the caudal thorax. The abdominal fat herniated into the pericardium and occupied the heart base. However, it did not enter circumferentially around the pericardium. The herniated tissue appears to measure 5.0 x 4.0 cm. Diaphragmatic hernia was present and measured 2.0 cm. The stomach was displaced. Normal cardiac function.
If respiratory distress under exercise is an issue then this is likely owing to pericardial diaphragmatic hernia and lack of adequate oxygenation of the lung fields owing to the herniation. However, many patients live normally with this type of hernia over a number of years. Therefore, other source of lethargy such as infectious disease, orthopedic disease, general inflammation or possible splenic related disease should be considered. The splenic enlargement is not explainable. Given the size of 1.4 cm, ultrasound-guided FNA would be indicated especially if any weight loss is present. Surgical consultation could be considered. However, it is debatable on whether surgery is absolutely necessary in this patient.