An 8-year-old, intact male Saluki was presented for generalized ADR, PU/PD and history of UTI. The patient had been treated with smz/tmp but this was discontinued due to suspected reaction to the medication. Abdominal radiographs showed a possible enlarged left kidney.
An 8-year-old, intact male Saluki was presented for generalized ADR, PU/PD and history of UTI. The patient had been treated with smz/tmp but this was discontinued due to suspected reaction to the medication. Abdominal radiographs showed a possible enlarged left kidney.
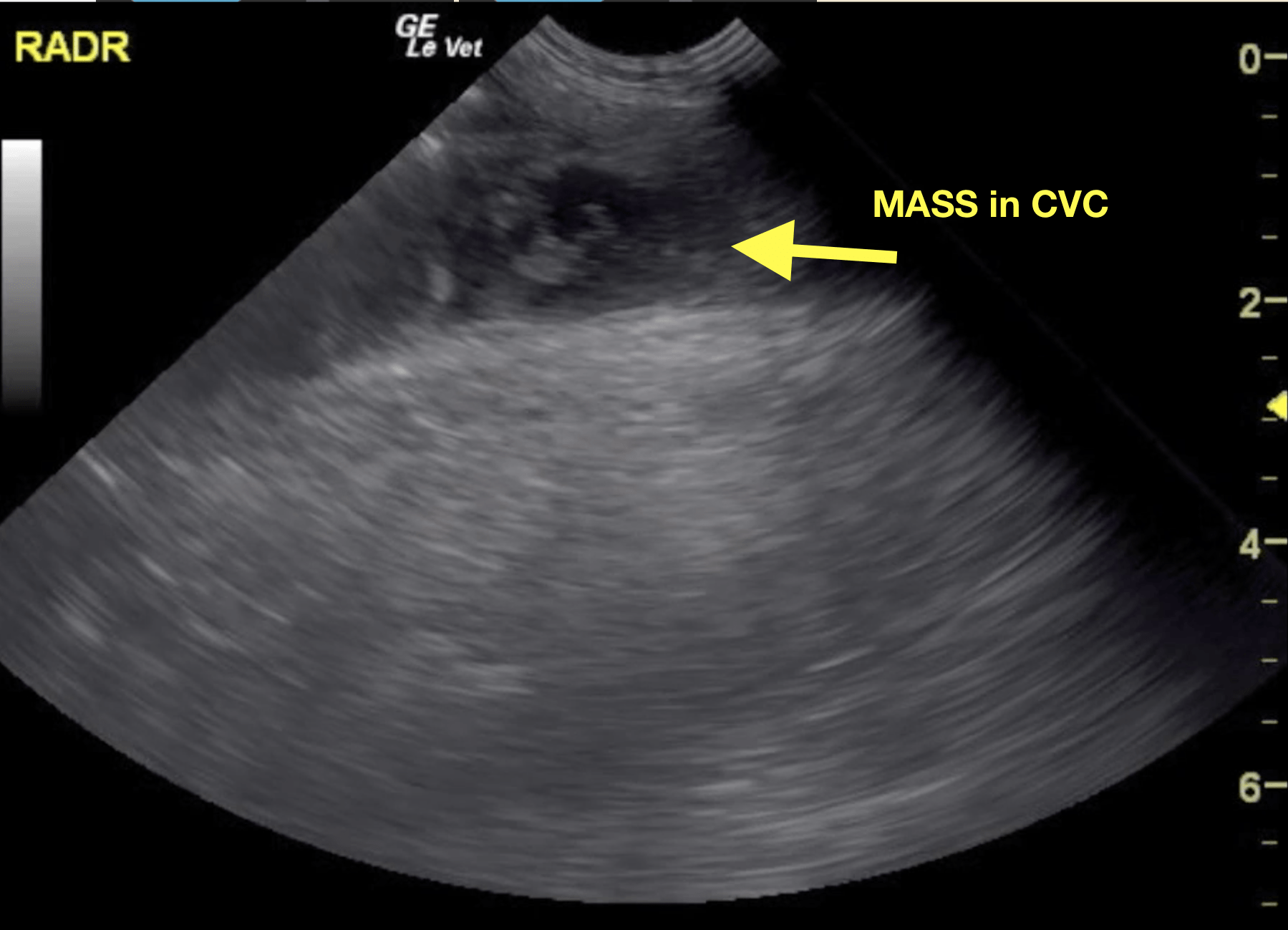
Right adrenal mass with vascular invasion and caudal vena cava syndrome.
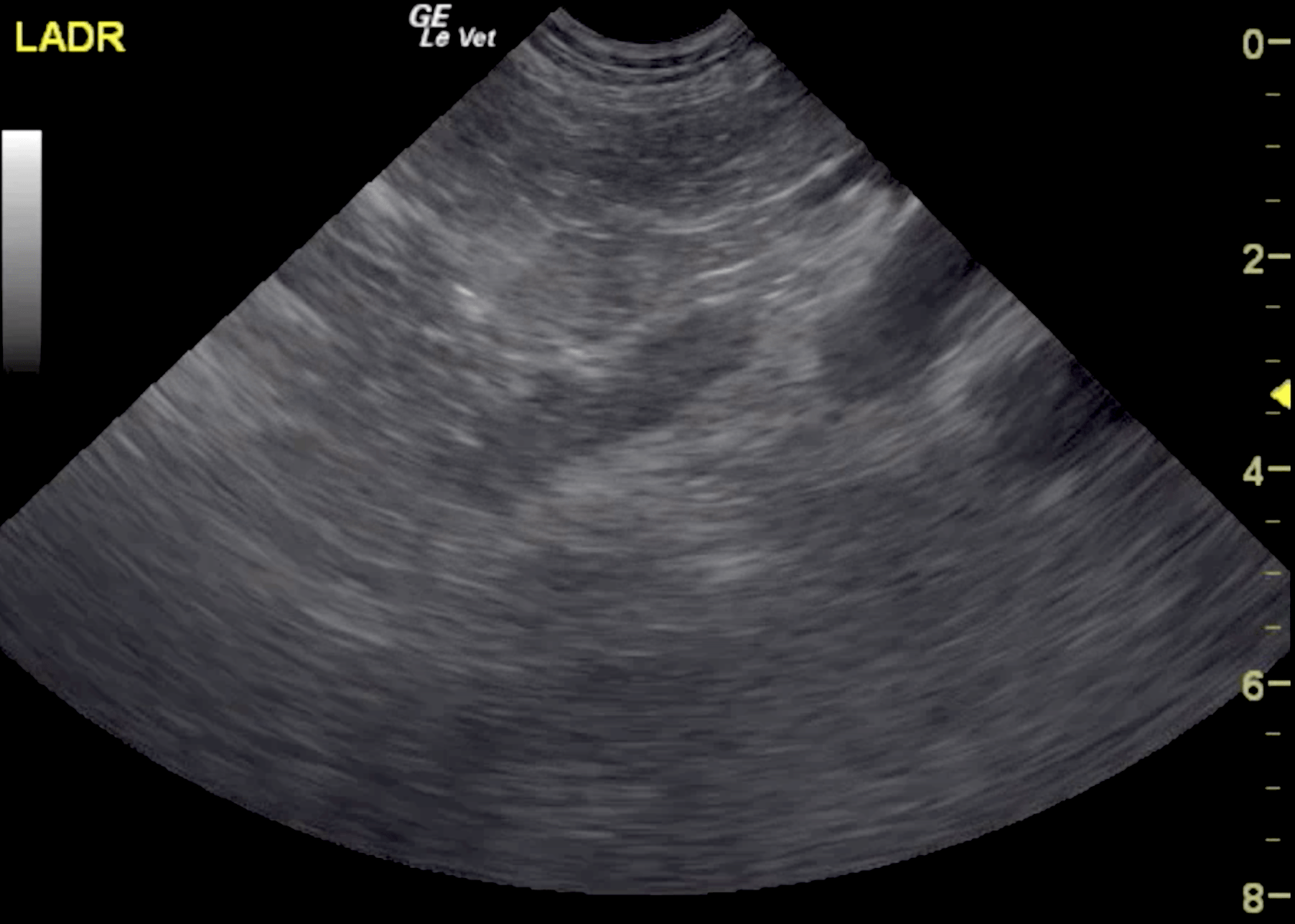
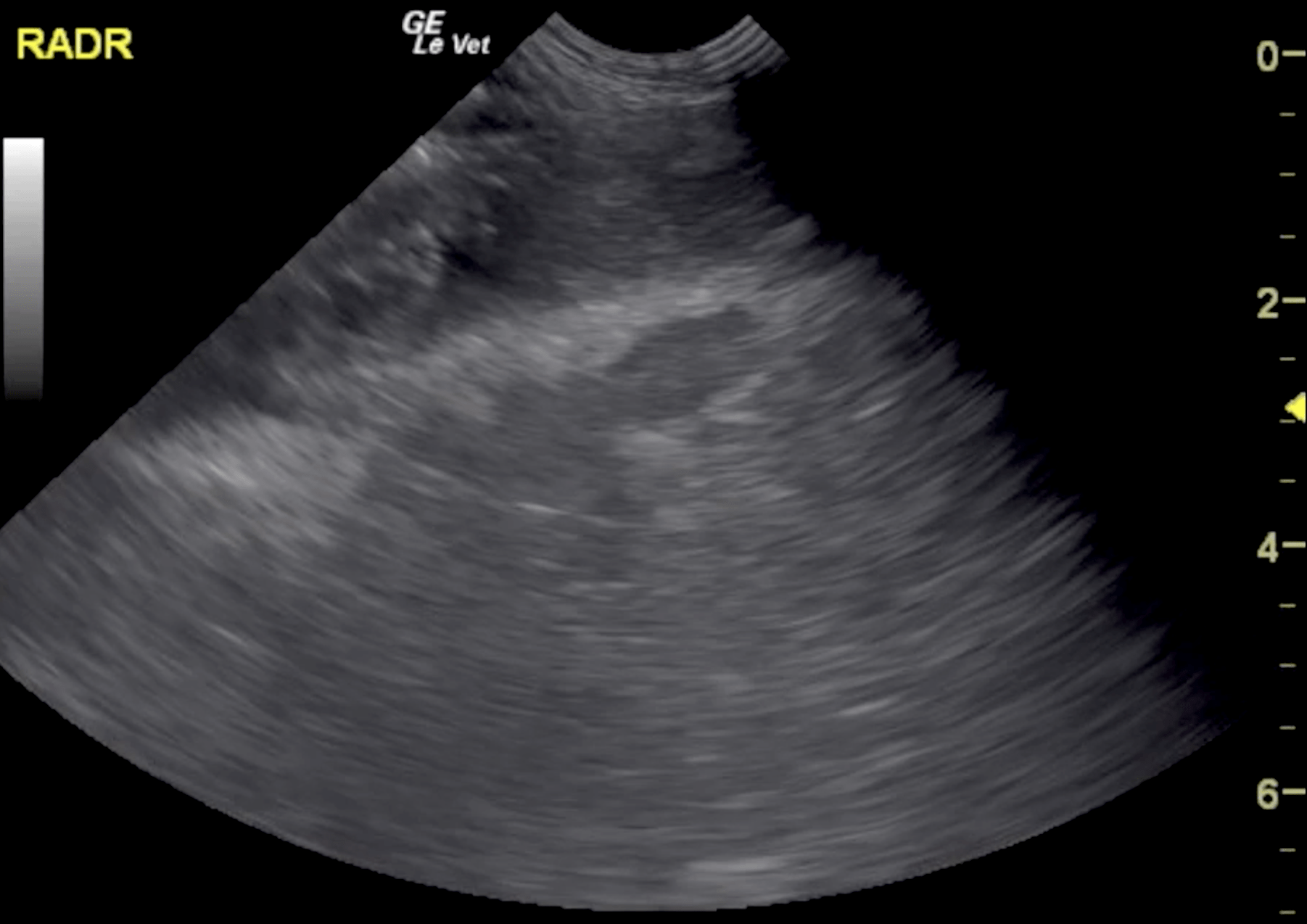
Both kidneys appear to be slightly swollen. However, the overall size and shape of the kidneys is within normal limits. The corticomedullary definition is slightly ill defined in both kidneys. The renal cortices present a mild overall increase in echogenicity. The renal and interlobar veins are moderately distended. The cranial pole of the right adrenal gland is mildly enlarged with ill defined margins. A stalk like tissue growth from the right adrenal gland invades the right phrenicoabdominal vein and connects to the caudal vena cava where it blends into a large hypoechoic heterogeneous vascularized mass, which fills the lumen of the caudal vena cava. An echogenic non-vascularized thrombus is seen caudal to the hypoechoic mass within the caudal vena cava. The caudal vena cava is distended caudal to the mass. The intravascular tumor and thrombus allow for marginal blood flow within the caudal vena cava only. The renal and adrenal veins are distended caudal to the mass. Right caudal pole measuring 0.74 cm in height. Left cranial and caudal pole measuring 0.74 and 0.74 cm in height respectively.
Findings were consistent with right adrenal mass with vascular invasion meeting neoplastic criteria. The vascular invasion is a sign of malignancy. Integrating the patient demographics, history and ultrasonographic findings, a pheochromocytoma is considered very likely. The vascular and renal congestion is considered a consequence of the tumor thrombus plugging the caudal vena cava (vena cava syndrome). The cranial extent of the intravascular component cannot be assessed fully. CT (including early and late phase post contrast studies) would be ideal for further definition and assessment of the resectability of the mass. Full laboratory work up is recommended to rule out Cushing’s/adenocarcinoma/other neoplasia even if considered far less likely, as well as serial blood pressure measurements. Measurements of catecholamines and metabolites in urine or plasma should be considered as well.